
What Is the ADHD ICD-10 Code?
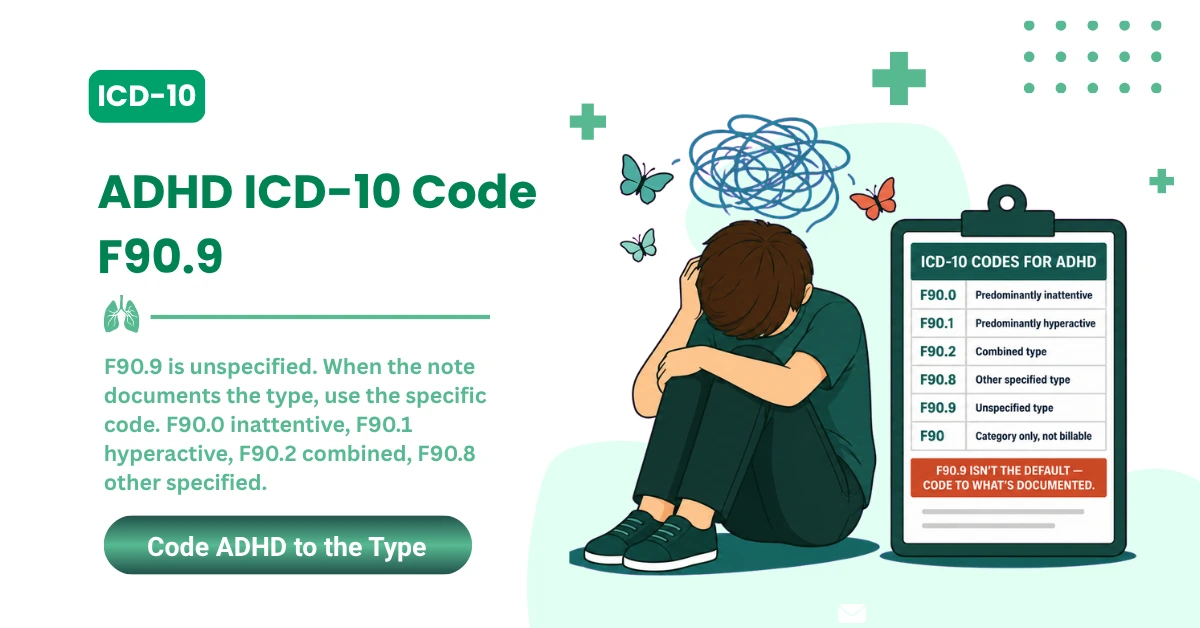
ADHD is reported in ICD-10-CM under the F90.- code family. The billable ADHD ICD-10 codes are F90.0, F90.1, F90.2, F90.8, and F90.9. F90.9 is the unspecified ADHD code, not the best default when documentation supports a more specific presentation.
Most practices don't lose ADHD revenue because someone forgot what F90.9 means. They lose it further down the line. The claim goes out with the wrong F90 code, or the note doesn't back up the code that got picked, or the service and the diagnosis don't match.
Denials also stack up when F90.9 becomes the house default, when a real comorbidity never makes it onto the claim, or when medical necessity reads thin. Those gaps live in documentation and workflow, which is where the fix has to start.
That's the gap MedSole RCM works in. We connect the diagnosis on the chart to a clean claim, then handle the denial follow-up, payment posting, and AR work that comes after. This guide walks the ADHD ICD-10 side of that, starting from the code itself.
|
One correction up front: F90.9 shows up everywhere as the ADHD diagnosis code, but it's only the unspecified one. For billing, the accurate answer is the whole F90.- family, and the specific code your note supports. |
If your ADHD claims keep getting delayed, denied, or underpaid, the sections below show where coding, documentation, and workflow usually break, and what to tighten first.
Key Takeaways for ADHD ICD-10 Billing in 2026
- ADHD lives under ICD-10-CM category F90.-, the attention-deficit hyperactivity disorder family. CDC/NCHS ICD-10-CM files host the official code set.
- F90 is a parent category, not the most specific billable code when an F90.x code applies.
- F90.0 reports predominantly inattentive ADHD.
- F90.1 reports predominantly hyperactive type.
- F90.2 reports combined type.
- F90.8 reports other specified ADHD.
- F90.9 reports ADHD only when the type isn't documented.
- Outpatient “rule out ADHD” should never be coded as confirmed ADHD.
- MedSole RCM helps practices cut ADHD coding gaps, denial risk, and aging AR, with medical billing at 2.99% of collections and credentialing at $99 per payer.
2026 Update: Which ICD-10-CM Code Set Applies to ADHD Claims Now?
For current 2026 dates of service, you bill from the FY2026 ICD-10-CM code set. The April 1, 2026 update applies through September 30, 2026, per CDC/NCHS ICD-10-CM files. Working from an outdated file is a quiet way to trigger rejections.
FY2027 files are already posted, but they apply to services and discharges beginning October 1, 2026. CMS ICD-10 resources maintain both the FY2026 and FY2027 update files, so the right set depends on your date of service, not the date you submit.
The ADHD F90 codes stay the working family for current ADHD diagnosis coding either way. Revalidate your code files for any date of service on or after October 1, 2026, and confirm nothing shifted before those claims go out.
|
2026 coding note: Use FY2026 ICD-10-CM codes for current dates of service through September 30, 2026. Revalidate against FY2027 files for dates of service on or after October 1, 2026. |
What Changed for ADHD Codes in FY2026?
For the F90 family, nothing meaningful changed based on the 2026 research at hand. No new ADHD subcodes, no retired ones. The value here isn't a code change to chase.
The value is discipline. You still have to bill from the current set, and you still have to pick the most specific F90.x code the documentation supports. That habit is what protects the claim, not a calendar update.
ADHD ICD-10 Code Table: F90.0, F90.1, F90.2, F90.8, and F90.9
Here's the full set of billable ADHD ICD-10 codes in one place. Coders and answer engines both want this as a clean table, so the descriptions below match the official ICD-10-CM wording and the note tells you when each one fits.
|
ICD-10 Code |
Official ADHD Description |
When Providers Use It |
Billing Note |
|---|---|---|---|
|
F90.0 |
ADHD, predominantly inattentive type |
Inattentive presentation or ADD-inattentive documentation |
Use when inattention is documented and hyperactivity isn't the main picture |
|
F90.1 |
ADHD, predominantly hyperactive type |
Hyperactive or hyperactive-impulsive presentation |
Use when hyperactivity or impulsivity is the dominant documented presentation |
|
F90.2 |
ADHD, combined type |
Both inattentive and hyperactive-impulsive presentation |
Use when the note supports both symptom clusters |
|
F90.8 |
ADHD, other type |
Other specified ADHD type |
Use when ADHD is specified but not captured by F90.0, F90.1, or F90.2 |
|
F90.9 |
ADHD, unspecified type |
ADHD confirmed but type not documented |
Use only when the record doesn't support a more specific type |
This isn't a fringe list. CMS's Psychiatry and Psychology Services coverage article lists F90.0, F90.1, F90.2, F90.8, and F90.9 in a real billing context, which is why payers expect the specific code rather than the parent.
Is F90 the ICD-10 Code for ADHD?
F90 is the category for attention-deficit hyperactivity disorders, not a code you bill on its own. For a claim, you almost always need a more specific billable F90.x code. That single step clears up most of the F90-versus-F90.x confusion payers flag.
Getting the code right only matters if it flows into a clean claim. MedSole's outsourced medical billing services connect accurate F90.x selection with clean claim submission, payer follow-up, and payment posting, so the specificity you documented actually survives to payment.
If you suspect F90.9 is showing up too often on your ADHD claims, a quick billing review can pinpoint where documentation and code selection need tightening before anything goes out the door.
What Each ADHD ICD-10 Code Means for Billing
Each F90 subcode maps to a documented presentation. Walk them one at a time, because the difference between them is exactly what a payer checks when a claim looks generic.
F90.0: ADHD, Predominantly Inattentive Type
F90.0 is the ICD-10-CM code for ADHD, predominantly inattentive type. Reach for it when the provider documents inattentive ADHD as the main presentation, the classic trouble sustaining focus, missed details, and disorganization without dominant hyperactivity.
Plenty of providers still write “ADD” out of habit. Billing follows the documented diagnosis and the current ICD-10-CM wording, so an inattentive presentation documented as ADD still codes to F90.0, not a separate legacy code.
F90.1: ADHD, Predominantly Hyperactive Type
For predominantly hyperactive-impulsive ADHD, the ICD-10-CM code is F90.1. Use it when hyperactive or impulsive symptoms drive the presentation and inattention isn't the headline. Search volume here is low, but the code matters for completeness and accuracy.
F90.2: ADHD, Combined Type
F90.2 is the ICD-10-CM code for ADHD, combined type. It applies when the note documents both inattentive and hyperactive-impulsive symptom patterns. This is a high-demand code, and payers see it often, so the documentation needs to show both clusters.
Questions like “what is the ICD-10 code for ADHD F90.2” come up constantly because combined type is the most common adult and pediatric presentation. When both symptom sets are in the chart, F90.2 is the specific, defensible choice.
F90.8: ADHD, Other Type
Other specified ADHD takes F90.8 in ICD-10-CM. It fits when ADHD is documented and specified, yet doesn't land cleanly in F90.0, F90.1, or F90.2. Keep this one tied strictly to what the record actually says.
F90.9: ADHD, Unspecified Type
F90.9 is the ICD-10-CM code for ADHD, unspecified type. It's billable, but it isn't a default. When the provider documents a specific presentation, a more specific code carries the claim better, which sets up the F90.9 section next.
Diagnosis codes exist to support the service you're billing. For evaluations, therapy, or medication-management visits, MedSole's mental health CPT codes guide explains how the common behavioral health CPT codes connect back to the diagnosis you selected.
When Should Providers Use F90.9 for ADHD Claims?
|
Quick answer: F90.9 is the ICD-10-CM code for ADHD, unspecified type. It fits when ADHD is confirmed but the provider doesn't document the presentation. If the record supports inattentive, hyperactive, combined, or other specified ADHD, use a more specific F90.x code. |
F90.9 Is Valid When ADHD Is Confirmed but the Type Isn't Documented
There's a right time for F90.9. When the provider confirms ADHD but the note never specifies inattentive, hyperactive, combined, or other specified type, F90.9 is the honest, correct code. It reflects exactly what the record supports, no more.
F90.9 Shouldn't Replace a More Specific ADHD Code
The problem starts when F90.9 stands in for a specific code. If the chart clearly documents the presentation, defaulting to unspecified ADHD understates what you know. Coders should code to the specificity the provider gave them, which keeps the claim clean for the payer.
Why Overusing F90.9 Can Create RCM Problems
Leaning on F90.9 can invite questions. Payers may ask for records, medical necessity can look softer, and claims can slow down while someone reviews the chart. None of that is guaranteed, but each becomes more likely as unspecified coding climbs.
Overuse can also weaken comorbidity capture and set up avoidable denials. When ADHD claims deny because the diagnosis, CPT code, or documentation don't line up, MedSole's denial management services find the root cause and recover revenue that was preventable in the first place.
Code assignment ultimately depends on provider documentation and specificity, a point the FY2026 ICD-10-CM Official Guidelines make plainly. That's the standard your coders should hold the chart to before a claim leaves the building.
If F90.9 shows up often in your ADHD claims, it's worth auditing whether the chart supports a more specific F90.x code before submission, rather than after a denial lands.
ADHD Documentation Requirements That Support Billing and Medical Necessity
Coding accuracy doesn't start with the coder. It starts with the note. When documentation is complete, the right ADHD ICD-10 code is obvious and the claim defends itself. When it's thin, even a correct code sits on shaky ground.
1. A Confirmed ADHD Diagnosis
Coders can't infer ADHD from symptoms alone. The provider has to document that ADHD exists as a diagnosis. Screening scores and complaints support the picture, but they don't replace a stated diagnosis, and a coder who guesses is a denial waiting to happen.
2. The ADHD Presentation or Type
The note should say which presentation applies: inattentive, hyperactive, combined, other, or unspecified. When that's missing or unclear, the coder's move is a provider query, not a default to F90.9. One clarifying question protects specificity and payment.
3. Functional Impairment and Medical Necessity
Claims read stronger when the chart shows how ADHD actually affects the patient, at school, at work, at home, or in daily functioning. That impairment is the backbone of medical necessity, and payers look for it before they look at anything clever.
4. Comorbidities That Affect Care
Anxiety, depression, learning disorders, sleep disorders, autism spectrum disorder, tics, and substance use often travel with ADHD. When they're documented and they shape treatment, they belong on the claim. Part 2 of this guide digs into the coding rules for them.
5. Medication Management and Treatment Monitoring
For medication visits, the note should capture response, side effects, refill barriers, treatment changes, and follow-up. This matters more for adults right now, where stimulant access is a real obstacle for a lot of patients.
The scale here is worth sitting with. CDC's adult ADHD report found 15.5 million U.S. adults had a current ADHD diagnosis in 2023, and about half were diagnosed in adulthood, which reshapes what “routine” ADHD documentation looks like.
The same body of data notes that 71.5% of adults taking stimulant medication reported trouble filling their prescription in the prior 12 months because the medication wasn't available. Documenting those refill barriers isn't busywork; it supports the visit.
|
Provider documentation checklist for ADHD billing: Confirm the diagnosis. Document the presentation. Support functional impairment. Code comorbidities that affect care. Match the diagnosis to the CPT-coded service. Clarify unspecified ADHD before submission when the record supports more detail. |
Documentation touches the whole claim lifecycle, from the note to the deposit. MedSole's revenue cycle management services connect documentation, coding, claim submission, payment posting, and AR follow-up into one workflow, so a strong note actually turns into paid revenue.
Diagnosing ADHD is a multi-step process with no single test, as CDC's diagnosis guidance describes, and sleep, anxiety, depression, and learning problems can mimic it. That overlap is exactly why the documented presentation carries so much billing weight.
A documentation and billing audit can show whether your ADHD claims are supported before they turn into denials, unpaid balances, or aging AR. It's cheaper to catch a thin note now than to appeal it in 90 days.
Can Providers Code “Rule Out ADHD” on Outpatient Claims?
|
Direct answer: For outpatient claims, “rule out ADHD” should not be coded as confirmed ADHD. If the diagnosis is uncertain, code the symptoms, signs, abnormal findings, or reason for the visit until the provider documents a confirmed ADHD diagnosis. |
This is where a lot of well-meaning teams slip. In outpatient coding, a suspected diagnosis isn't the same as a confirmed one. If the provider is still working the question, the claim has to reflect what's actually known at that visit.
Why “Rule Out ADHD” Shouldn't Be Billed as Confirmed ADHD
When a note says “rule out ADHD,” “possible ADHD,” or “working ADHD diagnosis,” the billing team shouldn't auto-assign F90.9. Outpatient rules ask you to code to the highest certainty for that encounter, and a maybe isn't a confirmed F90.x.
This mirrors the outpatient uncertainty rule in the FY2026 ICD-10-CM Official Guidelines, which direct coders away from reporting probable, suspected, or rule-out conditions as if they were confirmed. Certainty drives the code, not the working hypothesis.
What to Document Instead
Until ADHD is confirmed, the provider should document the presenting symptoms, the reason for the visit, any screening performed, the assessment status, and the follow-up plan. That record supports a real claim without overstating a diagnosis the chart can't yet defend.
The RCM Risk of Coding Too Early
Jumping to a confirmed code early invites payer review, medical necessity questions, and documentation mismatches. Then come corrected claims, denial follow-up, and aging AR, all for a code that got ahead of the chart. Patience here is cheaper than rework.
Solo and small practices feel this most, because documentation-to-claim alignment usually rides on one or two people. MedSole supports medical billing for private practices that need cleaner documentation review, accurate claim submission, and payer follow-up without standing up a full in-house billing team.
If your team is billing suspected ADHD as confirmed ADHD, a focused coding audit can stop the rework before claims ever reach the payer. One workflow fix usually clears the whole pattern.
ADHD Comorbidities, Excludes2 Notes, and Code Specificity
ADHD rarely shows up alone. Comorbidities change documentation, coding, treatment planning, and claim review, so they belong in any honest billing guide. This section stays in billing lane, not clinical advice, but the coding rules are worth knowing.
Excludes2 Doesn't Always Mean “Never Code Together”
Excludes2 is widely misread. It signals that the excluded condition isn't part of the coded condition, yet the patient can have both. When both are documented and both affect care, both may be coded, following the record and payer rules.
Several ADHD-adjacent Excludes2 categories come up often: anxiety disorders in F40.- and F41.-, mood disorders across F30 to F39, pervasive developmental disorders in F84.-, and schizophrenia in F20.-. Knowing they're Excludes2 keeps you from dropping a valid second code by reflex.
Common Comorbidities That Affect ADHD Claims
|
Comorbidity |
Why It Matters for Billing |
|---|---|
|
Anxiety disorders |
May affect treatment planning, medical necessity, and visit complexity |
|
Depression or mood disorders |
May require separate documentation and its own diagnosis capture |
|
Autism spectrum disorder |
May affect evaluation, therapy planning, and payer review |
|
Learning disorders |
May support the need for assessment, coordination, or therapy services |
|
Sleep disorders |
May mimic or worsen ADHD symptoms and affect clinical assessment |
|
Substance use disorders |
May affect medication management and risk documentation |
|
Tics or Tourette syndrome |
May affect treatment choice and monitoring |
RCM Point: Missed Comorbidities Can Understate Patient Complexity
When a documented comorbidity never reaches the claim, the story gets thinner than the visit was. That can understate medical necessity and, where it applies, affect risk adjustment or quality reporting. Capturing what's documented keeps the claim honest, without promising a bigger check.
ADHD claims often run through psychiatry, pediatrics, primary care, therapy, and behavioral health clinics. MedSole's specialty medical billing services support providers whose ADHD claims involve behavioral health and complex comorbidity documentation across exactly those settings.
|
Short answer: ADHD can be documented with comorbid conditions when the provider clearly documents them and they affect care, treatment, or management. Common examples include anxiety, depression, autism spectrum disorder, learning disorders, sleep disorders, tics, and substance use disorders. See NIMH's ADHD overview for clinical background. |
Comorbidity is a clinical call the provider makes and documents, not something a coder adds. CDC's clinical care guidance frames how coexisting conditions factor into ADHD care, and the coding always follows what the provider actually recorded.
When ADHD shows up alongside anxiety, depression, autism, learning disorders, or sleep problems, MedSole can help review whether the claim tells the full documented story before it goes out.
Common CPT Codes Billed With ADHD ICD-10 Codes
ICD-10-CM codes say why the patient is being treated. CPT codes say what service happened. For ADHD claims, both have to agree with the note, and this is where a simple diagnosis guide turns into real billing.
|
Plain-language rule: ADHD ICD-10 codes explain the diagnosis. CPT codes explain the service. For clean billing, the provider note should support both the selected F90.x diagnosis and the CPT-coded service on the same claim. |
||
|
CPT Code |
Service Type |
ADHD Billing Relevance |
|
90791 |
Psychiatric diagnostic evaluation |
Often used for the initial behavioral health evaluation when no medical services are included |
|
90792 |
Psychiatric diagnostic evaluation with medical services |
Often used when the psychiatric evaluation includes medical services |
|
96127 |
Brief emotional or behavioral assessment |
Commonly tied to ADHD screening or rating-scale workflows |
|
96130-96131 |
Psychological testing evaluation services |
May apply when psychological testing evaluation is documented |
|
96136-96137 |
Test administration and scoring |
May apply when testing is administered and scored |
|
90832 |
Psychotherapy, 30 minutes |
May apply when therapy is medically necessary and documented |
|
90834 |
Psychotherapy, 45 minutes |
Common behavioral health therapy visit duration |
|
90837 |
Psychotherapy, 60 minutes |
Longer psychotherapy visit when the time is supported |
|
99213-99214 |
E/M follow-up |
May apply to medication management or follow-up when documentation supports the level |
Why CPT and ICD-10 Alignment Matters
Think of it as two halves of one claim. ICD-10 supports the diagnosis and medical necessity, CPT reports the service, and the note has to connect them. A perfect diagnosis code with a mismatched service still reads as a problem to the payer.
Diagnosis alone never guarantees coverage, either. CMS is explicit that correct use of a listed ICD-10-CM code doesn't automatically assure payment, because the service still has to be reasonable, necessary, and meet coverage criteria, a point reinforced across its Psychiatry and Psychology Services guidance.
For evaluation-heavy ADHD workups, the code details do the heavy lifting. Our CPT code 90791 billing guide covers the diagnostic evaluation without medical services, which is the common entry point for a first ADHD visit with a non-prescribing provider.
When the evaluation includes medical services like a prescribing decision, the code shifts. The CPT code 90792 billing guide walks that distinction, and getting it right is the difference between full payment and a downcode on audit.
Ongoing ADHD therapy usually lands on the 45-minute code. Our CPT code 90834 billing guide covers the time documentation and payer rules that keep those routine visits clean, since they make up the bulk of behavioral health claim volume.
CPT itself is maintained by the AMA, and the AMA CPT overview is the authority for how these codes are defined and updated each year. Pairing the right CPT with the right F90.x code is the whole game for ADHD billing.
For providers weighing an affordable medical billing company for behavioral health claims, MedSole RCM offers medical billing at 2.99% of collections. That framing matters more than any “best in market” label, because the rate is the part you can actually verify.
If ADHD-related CPT and ICD-10 pairing is generating rejections, a coding-path review can catch the mismatch before those claims turn into denials or aging AR.
Common ADHD Claim Denials and How to Prevent Them
Most ADHD claim problems are preventable, and they cluster around a handful of triggers. Here's the short list of what goes wrong, why it happens, and the step that keeps it off your denial report.
|
Denial or Delay Trigger |
Why It Happens |
Prevention Step |
|---|---|---|
|
F90.9 used when a specific type is documented |
The claim lacks code specificity |
Use F90.0, F90.1, F90.2, or F90.8 when supported |
|
Rule-out ADHD coded as confirmed |
Diagnosis wasn't confirmed for outpatient coding |
Code the highest certainty known for the encounter |
|
CPT and ICD-10 mismatch |
The diagnosis doesn't support the billed service |
Match the note, the diagnosis, and the CPT code |
|
Missing functional impairment |
Medical necessity is unclear |
Document school, work, home, social, or daily-life impact |
|
Missing comorbidity capture |
Patient complexity is understated |
Code documented conditions that affect care |
|
Prior authorization missed |
The payer required authorization for testing or services |
Verify benefits and payer rules before the service |
|
No follow-up on a denied claim |
The denial sits unresolved in AR |
Track, appeal, correct, or rebill within payer timelines |
Why ADHD Claims Need Front-End Review
Most of these denials are born before submission. Thin documentation, a vague diagnosis code, a missed authorization, or a weak CPT pairing all create downstream AR. Catching them at the front end costs minutes; catching them after denial costs weeks.
How MedSole Prevents Avoidable ADHD Billing Issues
The fix is a workflow, not a hero coder. MedSole runs eligibility and benefits review, an authorization check when it's required, and a coding and documentation review before anything is scrubbed and submitted. The goal is a clean first pass.
That work starts with coverage. MedSole's verification of benefits services confirm eligibility and payer rules up front, so an ADHD testing or therapy claim doesn't die on a benefit limit or a plan requirement nobody checked.
Testing and some services need sign-off first. MedSole's prior authorization services handle that step before the visit, which closes the single most expensive gap in ADHD testing claims, the authorization that was required and never obtained.
When a claim still denies, it can't sit. MedSole's AR follow-up services track, appeal, correct, and rebill within payer timelines, so a denied ADHD claim gets worked instead of quietly aging past the point of recovery.
If ADHD claims are getting denied, delayed, or left in AR, a claim-path review from eligibility to payment posting can show exactly where revenue is leaking, and how much of it is recoverable.
How MedSole RCM Helps Providers Bill ADHD Claims More Cleanly
ADHD coding is one piece of the revenue cycle, not the whole thing. A clean claim depends on eligibility, documentation, coding, CPT pairing, authorization, submission, denial management, payment posting, and AR follow-up all working together.
MedSole RCM offers medical billing at 2.99% of collections and provider credentialing at $99 per payer. That pricing is transparent, tied to collected revenue, and built for behavioral health and private practices comparing affordable billing partners.
Medical Billing at 2.99% of Collections
For providers comparing affordable medical billing companies, MedSole RCM offers medical billing at 2.99% of collections, so the billing cost stays tied to collected revenue instead of inflated claim volume. It's a provider-friendly structure, not a per-claim meter.
Credentialing at $99 per Payer
For providers comparing credentialing companies, MedSole offers provider credentialing at $99 per payer, which helps practices get enrollment support without heavy setup costs. Transparent per-payer pricing keeps a growing panel from turning into a growing invoice.
Full RCM Support for Behavioral Health and Medical Practices
Beyond coding, MedSole handles eligibility verification, prior authorization, coding review, claim submission, denial management, AR follow-up, and provider enrollment. One team owns the workflow, so behavioral health revenue isn't split across vendors who never talk.
Clean payment posting closes that loop. MedSole's payment posting services reconcile what actually paid against what was billed, which is how underpayments and short-pays on ADHD claims get caught instead of quietly written off.
Getting paneled comes first for new providers. MedSole's provider credentialing services manage enrollment at $99 per payer, so an ADHD-focused clinician can start billing without months of setup friction slowing the first claim.
If you want a billing partner that understands ADHD claims, behavioral health coding, denials, and payer follow-up, you can request a free billing analysis from MedSole RCM and see where your current process is leaking revenue.
FAQs About ADHD ICD-10 Codes and Billing
Short, direct answers to the questions providers and billing teams ask most about ADHD ICD-10 codes. Each one stands on its own, so you can lift the answer you need without reading the rest.
What is the ICD-10 code for ADHD?
ADHD is coded under the ICD-10-CM F90.- family. The billable ADHD codes are F90.0, F90.1, F90.2, F90.8, and F90.9. F90.9 is unspecified ADHD, not the only ADHD diagnosis code. For a specific presentation, the more accurate answer is the matching F90.x code.
Is F90.9 the main ADHD diagnosis code?
F90.9 is the unspecified ADHD diagnosis code. It shows up often in search results, but it's meant for cases where ADHD is confirmed and the provider doesn't document the type. When the record supports a specific presentation, a more specific F90.x code is the correct choice.
What is F90.0?
F90.0 is the ICD-10-CM code for attention-deficit hyperactivity disorder, predominantly inattentive type. Use it when the provider documents inattentive ADHD, or an ADD-inattentive presentation, and the documentation supports that type as the main clinical picture for the visit.
What is F90.1?
F90.1 is the ICD-10-CM code for attention-deficit hyperactivity disorder, predominantly hyperactive type. Use it when the provider documents hyperactive or hyperactive-impulsive ADHD as the dominant presentation, with inattention playing a secondary role in the clinical picture.
What is F90.2?
F90.2 is the ICD-10-CM code for attention-deficit hyperactivity disorder, combined type. It applies when the provider documents both inattentive and hyperactive-impulsive features that together support a combined presentation. It's the most common ADHD presentation across both pediatric and adult patients.
What is F90.8?
F90.8 is the ICD-10-CM code for attention-deficit hyperactivity disorder, other type. Use it when the provider documents another specified ADHD type that isn't best represented by F90.0, F90.1, or F90.2. Keep it tied to what the record specifies.
What is the difference between F90.2 and F90.9?
F90.2 is combined-type ADHD, used when both inattentive and hyperactive-impulsive features are documented. F90.9 is unspecified ADHD, used when the provider confirms ADHD but doesn't document the type. When the record supports the detail, F90.2 is the more specific and defensible code.
Can you code rule-out ADHD?
For outpatient claims, rule-out ADHD shouldn't be coded as confirmed ADHD. When the provider documents possible, suspected, probable, or rule-out ADHD, code the symptoms, signs, abnormal findings, or reason for the visit until ADHD is confirmed. Certainty for that encounter drives the code.
Can ADHD be coded with anxiety or depression?
Yes, when anxiety, depression, or another condition is documented by the provider and affects care, treatment, or management. ADHD commonly appears with behavioral health comorbidities, so the documentation should show how each condition shaped the encounter before a second code goes on the claim.
What CPT codes are commonly billed with ADHD ICD-10 codes?
Common CPT codes connected to ADHD care include 90791, 90792, 96127, 96130, 96131, 96136, 96137, 90832, 90834, 90837, 99213, and 99214. The correct code depends on the service that was actually performed and documented, not on the diagnosis alone.
Does ICD-11 change ADHD billing in the United States?
No. ICD-11 is used internationally, but the United States still bills diagnoses under ICD-10-CM. Providers should use ICD-10-CM for U.S. claims and watch official CMS and CDC/NCHS updates for any future transition guidance before changing anything in their workflow.
Who can help providers with ADHD billing and credentialing?
MedSole RCM helps providers with ADHD billing, behavioral health claims, denial management, AR follow-up, payment posting, and provider enrollment. MedSole offers medical billing at 2.99% of collections and credentialing at $99 per payer. See MedSole's medical billing and credentialing services for the full workflow.
Coding rules shift with each fiscal year, so anchor to primary sources. CMS ICD-10 resources host the current code files and update timing, and a free billing analysis can map those rules onto your specific ADHD claims.
Final Billing Takeaway for Providers
Pull it together and the picture is simple. ADHD is reported under the F90.- code family, and the correct F90.x code depends on what the provider documented, not on habit or a default to unspecified.
F90.9 isn't the best pick when a specific type is on the chart. CPT and ICD-10 alignment supports medical necessity, and comorbidities belong on the claim when they're documented and relevant to care.
Most ADHD billing problems turn out to be RCM workflow problems. They live in eligibility, documentation, coding, authorization, and follow-up, which is also where they get solved, well before a denial ever prints.
That's the work MedSole owns end to end, from the ADHD ICD-10 code to the deposit. Our outsourced medical billing services cover billing, credentialing, denials, AR, and payment posting so your team can stay focused on patients.
MedSole RCM offers medical billing at 2.99% of collections and provider credentialing at $99 per payer. If your practice wants cleaner ADHD claims, fewer preventable denials, and a more affordable RCM partner, request a free billing analysis.