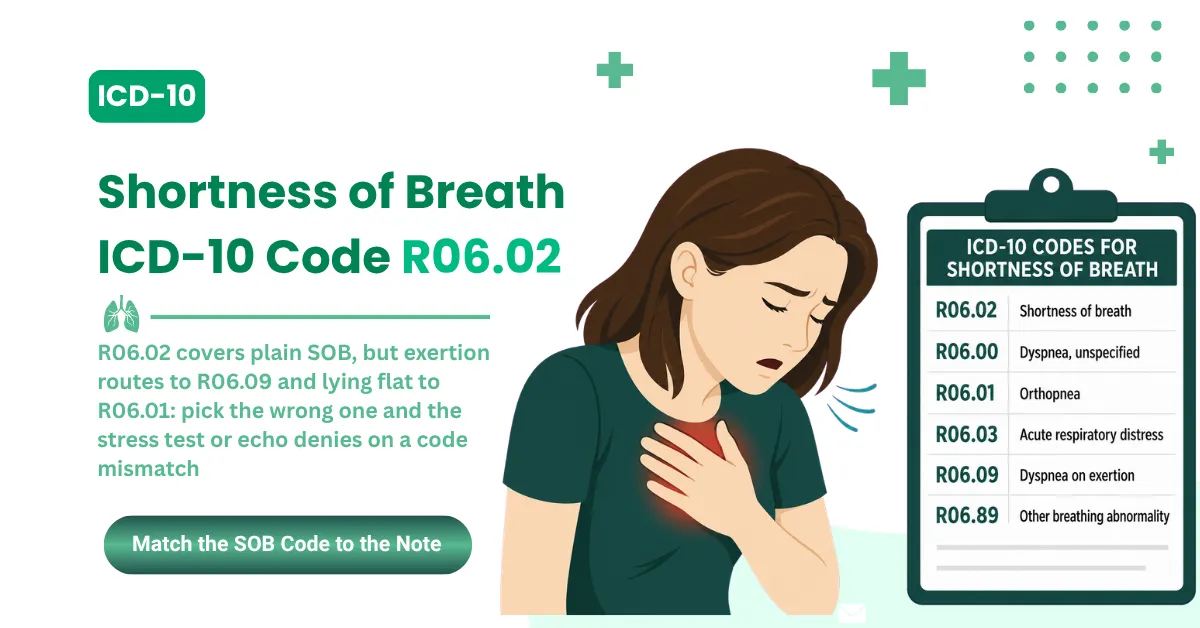

R06.02 Is the ICD-10-CM Code for Shortness of Breath, and Three Common Mapping Errors Are Costing Providers Money
R06.02 is the ICD-10-CM code for shortness of breath (SOB). It's a billable, specific code valid for HIPAA-covered transactions from October 1, 2025 through September 30, 2026 under the FY2026 code set.
The shortness of breath ICD-10 code applies when SOB is the documented symptom and the provider hasn't confirmed an underlying cause such as COPD, asthma, or congestive heart failure.
Several sources ranking for the shortness of breath ICD-10 code get it wrong. Some map R06.02 to shortness of breath on exertion, and others describe it as orthopnea. Both designations are incorrect, and both trigger claim denials. Exertional dyspnea belongs to R06.09, and orthopnea belongs to R06.01.
The wrong code here can also pull medical necessity review onto the services billed alongside it.
R06.02 is billable and specific. The parent code R06.0 (Dyspnea) is not. Submit R06.0 without the fifth character and the clearinghouse kicks it back on an automated edit, no matter how clean the documentation is. R06.1 (Stridor) is a separate non-billable parent. Always use the five-character subcode: R06.02, R06.00, or R06.09.
Related breathing difficulty codes, used when the breathing pattern is documented:
|
Code |
When to use |
|---|---|
|
R06.02 |
General SOB or difficulty breathing when no cause is confirmed. The most commonly billed code in this family. |
|
R06.00 |
Dyspnea, unspecified. Use when “dyspnea” is documented with no position, context, or qualifier. |
|
R06.01 |
Orthopnea. SOB that occurs when lying flat, common in heart failure. Requires positional documentation. |
|
R06.03 |
Acute respiratory distress. Severe, sudden breathing difficulty meeting clinical severity criteria. Not all acute-onset SOB qualifies. |
|
R06.09 |
Other forms of dyspnea. Includes dyspnea on exertion. Use when the provider documents SOB with physical activity. |
|
R06.89 |
Other abnormalities of breathing. For documented breathing abnormalities that don't fit the categories above. |
Billability rule: R06.0 and R06.1 are parent codes. They're never billable. Assign the specific five-character subcode every time. The clearinghouse rejects R06.0 as a standalone diagnosis before the claim reaches clinical review.
Shortness of breath is billable as a principal diagnosis. The SOB ICD-10 code R06.02 can carry a HIPAA-covered claim on its own when SOB is the documented reason for the visit and no underlying cause is confirmed.
AAPC's Codify lists R06.02 under code range R06 (Abnormalities of Breathing) in Chapter 18, a medical classification under WHO authority (aapc.com/codes/icd-10-codes/R06.02).
The CDC ICD-10-CM Browser Tool confirms the ICD-10 code for shortness of breath as billable and specific in the Symptoms, Signs and Abnormal Clinical Findings chapter, R00 to R99 (icd10cmtool.cdc.gov).
Providers in internal medicine, emergency medicine, cardiology, and pulmonology submit R06.02 on daily claims. Accuracy at the code level decides whether those claims clear or bounce. MedSole RCM's medical billing services for internal medicine and emergency medicine manage SOB encounter billing at 2.99% of collections with no setup fees.
FY2026 ICD-10-CM Update: The Two Release Windows That Determine Whether Your SOB Claims Clear
Most practices loaded the October 1, 2025 ICD-10-CM release at the start of the fiscal year and never touched it again. The April 1, 2026 mid-year release replaced that version. Bill a June 2026 date of service off the October files, and R06.02 can reject as an invalid code even when it's clinically correct.
The CDC and NCHS publish ICD-10-CM on a dual release cycle for FY2026. The October 1, 2025 release covers dates of service from October 1, 2025 through March 31, 2026.
The April 1, 2026 release, stamped “Updated April 1, 2026,” governs dates of service from April 1, 2026 through September 30, 2026. As of June 10, 2026, that April release is the operative code set. If you're checking the shortness of breath ICD-10 code against a current claim, R06.02 stays valid under it.
April 2026 compliance check: For any SOB claim with a date of service after April 1, 2026, confirm your practice management system loaded the FY2026 April release. Running a June 2026 encounter off the October files produces invalid-code rejections at the clearinghouse even when R06.02 is the correct clinical code.
The ICD-10 code for shortness of breath hasn't changed in the April update. R06.02 keeps the same description, billable status, and Chapter 18 classification. R06.02 has been billable since FY2016. The April release adjusted code file structure and guideline wording, not the R06 family itself.
The CDC has posted FY2027 ICD-10-CM files effective October 1, 2026. The R06 family, R06.02 through R06.89, stays unchanged in that release. Billing workflows that use R06.02 for shortness of breath hold through at least September 30, 2027.
|
ICD-10 code |
Description |
Effective date (FY2026) |
|---|---|---|
|
R06.02 |
Shortness of breath |
October 1, 2025 |
|
R06.00 |
Dyspnea, unspecified |
October 1, 2025 |
|
R06.01 |
Orthopnea |
October 1, 2025 |
|
R06.03 |
Acute respiratory distress |
October 1, 2025 |
|
R06.09 |
Other forms of dyspnea |
October 1, 2025 |
|
R06.89 |
Other abnormalities of breathing |
October 1, 2025 |
For teams managing broader respiratory and cardiovascular decisions, MedSole's ICD-10 billing guides for healthcare providers cover the codes that matter across internal medicine, cardiology, pulmonology, and emergency medicine.
The CDC and NCHS ICD-10-CM Files page documents the dual FY2026 release schedule and confirms R06.02 is unchanged in both the October 2025 and April 2026 releases (cdc.gov/nchs/icd/icd-10-cm/files.html).
CMS confirms the April 1, 2026 release at cms.gov/medicare/coding-billing/icd-10-codes.
R06.02, R06.00, or R06.09: Which Shortness of Breath Code Does Your Claim Actually Need?
Three R06 codes cover the breathing-difficulty symptom space, and picking the wrong shortness of breath ICD-10 code is what turns a clean encounter into a denial.
The Clinical Documentation Term Drives the Code, Not the Symptom Alone
The provider's exact documented term, not the clinical picture, decides which code is correct. ICD-10-CM coding follows documentation. When the provider writes “shortness of breath” or “SOB” with no qualifier, R06.02 is correct.
A note that says “dyspnea” alone points to R06.00, though both hold up with unqualified documentation. A note that says “dyspnea on exertion,” “SOB with activity,” or “exertional dyspnea” points to R06.09, not R06.02.
Payers run more claims through NLP-driven validation every year. A chart that documents “dyspnea on exertion” paired with R06.02 creates a documentation-to-code mismatch, and that mismatch flags during pre-payment review.
Documentation alignment rule: The diagnosis code has to match the exact language in the provider's assessment. If the note reads “dyspnea on exertion” and the claim shows R06.02, automated payer validation catches the mismatch and raises CO-16 denial risk.
R06.09 Is the Exertional Dyspnea Code, Not R06.02
This is the most common coding error on this topic, and it's generating real denials for providers who follow the wrong guidance on other billing sites.
The code structure leaves no ambiguity. R06.09 (Other forms of dyspnea) covers dyspnea on exertion per the ICD-10-CM Alphabetic Index. The current Google AI Overview lists R06.09 as the code that includes shortness of breath on exertion and physical activity.
The CDC ICD-10-CM Browser Tool routes “dyspnea on exertion” to R06.09. R06.02 covers general, unspecified shortness of breath, not exertion-specific presentations.
Exertion coding correction: When the provider documents SOB or dyspnea during physical activity, walking, stairs, or exercise, use R06.09, not R06.02. Coding R06.02 for documented exertional dyspnea is a specificity violation that can trigger medical necessity review on diagnostic testing.
Submit R06.02 on a claim where the notes document exertional dyspnea and the procedures include a stress test (CPT 93015) or pulmonary function test (CPT 94010), and the payer expects R06.09 as the linked diagnosis. Mismatched procedure-diagnosis pairs draw CO-4 denials on those high-value studies.
The Complete R06 Family Decision Guide
|
Clinical documentation |
Provider writes |
Correct code |
Incorrect code |
Billing risk of wrong code |
|---|---|---|---|---|
|
General breathing difficulty, no cause identified |
“shortness of breath,” “SOB,” “difficulty breathing” |
R06.02 |
R06.00 |
Minor. R06.00 is less specific but defensible |
|
Dyspnea without qualification |
“dyspnea,” “dyspnea NOS” |
R06.00 |
R06.02 |
Minor. Both defensible with unqualified notes |
|
SOB or dyspnea during physical activity |
“dyspnea on exertion,” “SOB with activity,” “DOE” |
R06.09 |
R06.02 |
CO-4 denial when paired with stress test or PFT |
|
SOB when lying flat, improves sitting up |
“orthopnea,” “can't lie flat,” “sleeps on pillows” |
R06.01 |
R06.02 |
Misrepresents severity, affects inpatient DRG |
|
Severe sudden breathing difficulty |
“acute respiratory distress” meeting criteria |
R06.03 |
R06.02 |
DRG miscoding inpatient, necessity risk outpatient |
|
Breathing abnormality not matching above |
“paradoxical breathing,” “Cheyne-Stokes” |
R06.89 |
R06.09 |
CO-16 if notes contradict the generic code |
Quick reference:
-
“shortness of breath” with no qualifier: R06.02
-
“dyspnea” with no qualifier: R06.00
-
“dyspnea on exertion” or “SOB with activity”: R06.09
-
“orthopnea” or “SOB lying flat”: R06.01
-
“acute respiratory distress”: R06.03
-
other specified breathing abnormality: R06.89
The CDC ICD-10-CM Browser Tool routes “dyspnea on exertion” to R06.09, confirming it as the exertional dyspnea code (icd10cmtool.cdc.gov).
When R06.02 Gets Replaced: Co-Coding Protocols for Heart Failure, COPD, Post-COVID, and Pregnancy
The Symptom-to-Disease Transition Rule: When R06.02 Has to Stop
Per the FY2026 ICD-10-CM Official Guidelines (Updated April 1, 2026, CMS and NCHS), symptom codes fit only until a definitive diagnosis is established. Once the provider documents a confirmed underlying diagnosis, the disease code replaces R06.02 as the primary code, or drops it entirely when SOB is a symptom routinely tied to that disease.
Code the confirmed disease first. The shortness of breath ICD-10 code stays as a secondary code only when the SOB is separately evaluated and managed, not when it's a manifestation of the primary condition.
R06 also carries Type 1 Excludes notes, and those generate automatic claim rejections when violated. A Type 1 Excludes pairing means two codes can't sit on the same claim. Never combine R06.02 with J80 (Acute respiratory distress syndrome), J96.x (Respiratory failure), R09.2 (Respiratory arrest), or P22.x (Newborn respiratory codes).
Type 1 Excludes rule: Pairing R06.02 with J80, J96.x, or R09.2 on the same claim triggers an automatic clearinghouse edit rejection. The claim fails before a human reviewer sees it, no matter the documentation quality.
The Co-Coding Scenarios That Come Up Most on SOB Claims
|
Confirmed condition |
Primary code |
R06.02 secondary? |
Co-coding note |
|---|---|---|---|
|
COPD exacerbation |
J44.1 |
No, SOB is integral |
COPD exacerbation includes SOB by definition; a separate R06.02 draws redundancy edits |
|
Congestive heart failure |
I50.9 or specific I50 subcode |
Only if separately evaluated |
If SOB is the main reason for the visit and CHF is confirmed, sequence CHF first |
|
Pneumonia, unspecified |
J18.9 |
No, SOB is integral |
Pneumonia includes respiratory symptoms by definition |
|
Asthma with exacerbation |
J45.901 |
No, SOB is integral |
Code the asthma exacerbation directly |
|
Post-COVID condition |
U09.9 + R06.02 |
Yes, as secondary |
U09.9 first, R06.02 second; add Z86.16 with prior confirmed COVID history |
|
GERD with dyspnea |
K21.9 + R06.02 |
Yes, if separately documented |
When GERD drives respiratory symptoms, code both if both are addressed |
|
Pulmonary embolism |
I26.x |
No, SOB is integral |
Code the PE directly; R06.02 isn't appropriate as an add-on |
|
Anxiety disorder with dyspnea |
F41.x |
Consider R06.02 secondary |
Only if the provider separately addresses the respiratory symptom |
When GERD is confirmed as the cause of respiratory symptoms, the GERD ICD-10 code K21.9 governs the primary billing decision, and R06.02 drops in favor of the gastrointestinal cause.
In post-stroke and elderly patients with aspiration risk, SOB often co-occurs with documented swallowing dysfunction. When both are separately addressed, report the dysphagia ICD-10 code R13.10 alongside R06.02.
Nocturnal SOB in heart failure patients creates documented sleep disruption. When the provider separately addresses the sleep disturbance, the insomnia ICD-10 code G47.00 may be reported alongside the cardiac codes.
Heart failure patients with SOB can show hepatic congestion and elevated transaminases. When that's separately addressed, report the ICD-10 code for transaminitis R74.01 alongside the cardiac codes.
Post-COVID Shortness of Breath: The Three-Code Protocol No Competitor Covers
Post-COVID dyspnea is a 2025-2026 billing reality that internal medicine, primary care, and pulmonology practices see weekly. No editorial RCM source on this topic has built a dedicated coding section for it. When the provider confirms post-COVID condition with shortness of breath as a residual symptom, use three codes:
-
U09.9, Post-COVID-19 condition, unspecified, as the primary code for the post-COVID status
-
R06.02, Shortness of breath, as the secondary code for the active respiratory symptom
-
Z86.16, Personal history of COVID-19, as the tertiary code when prior confirmed COVID is in the record
Post-COVID SOB sequencing: U09.9 first, R06.02 second, Z86.16 third. Don't use U07.1 (active COVID-19) for a post-COVID encounter unless the provider documents a current active infection. Coding U07.1 for a residual post-COVID respiratory symptom is an incorrect assignment that creates audit exposure.
The FY2026 ICD-10-CM Official Guidelines (Updated April 1, 2026) list R06.02 as an appropriate symptom code for unconfirmed COVID-19 presentations (cms.gov/medicare/coding-billing/icd-10-codes).
SOB in Pregnancy and Less Common Scenarios
For shortness of breath in pregnancy with no confirmed underlying cause, use R06.02 alongside the obstetric encounter code (Z34.x for supervision of pregnancy). If SOB stems from a confirmed pregnancy complication, code the O-series complication first. R06.02 alone fits physiologic dyspnea of pregnancy documented without a pathologic cause.
Both acute and chronic shortness of breath use R06.02, since ICD-10-CM has no separate acute or chronic subcodes inside it. Documentation captures the distinction through the onset timeline, which supports medical necessity for the level of workup billed.
Once U07.0 (Vaping-related disorder) is assigned as the principal diagnosis, associated SOB isn't coded separately under the FY2026 Official Guidelines. That's an explicit guideline instruction no competitor on this topic has flagged.
What Your Provider Note Has to Contain to Make an SOB Claim Audit-Proof
The Clinical Timeline That Changes How Payers Review SOB Claims
ICD-10-CM doesn't split acute from chronic shortness of breath by code, but CMS reviewers and payers use the documented timeline to judge medical necessity on a shortness of breath ICD-10 claim.
Per NIH and NCBI StatPearls (Updated December 2025), dyspnea sorts by onset:
-
Acute: develops over hours to days. Supports higher-level E/M and diagnostic testing necessity.
-
Subacute: evolves over several days to four weeks. Supports a systematic workup.
-
Chronic: persists beyond four weeks. Supports ongoing management and specialist referral.
The timeline has to appear in the provider note. “Patient reports shortness of breath” with no onset is the single most common medical necessity denial trigger for R06.02 claims. CMS post-payment review flags symptom-only codes that lack documented onset, duration, and clinical rationale.
Timeline documentation rule: State the onset in exact terms. “Patient reports shortness of breath for three days, worsening with exertion” is defensible. “Patient has SOB” is not. The timeline decides whether the workup you billed is justified.
The Note Elements CMS Auditors Look for in R06.02 Claims
Required documentation for audit-proof R06.02 claims:
-
Onset and duration, in exact days or weeks, not “recent” or “new”
-
Context: at rest, exertional, positional, or nocturnal
-
Severity: mild, moderate, severe, or functional language such as “speech-limiting dyspnea”
-
Objective data: respiratory rate, oxygen saturation at rest, and saturation with ambulation when relevant
-
Associated symptoms: chest pain, cough, fever, wheezing, edema, or syncope
-
Clinical impression: what the provider is evaluating and why, even before the cause is confirmed
-
Workup justification: the clinical reason each test was ordered, not the bare “chest X-ray ordered”
-
Response to treatment: whether oxygen therapy improved saturation, when applicable
A strong note reads like this: “Patient reports acute onset shortness of breath for two days, worsening with exertion, denies chest pain. Oxygen saturation 88% on room air, improving to 95% with supplemental oxygen. Respiratory rate 24. Chest X-ray ordered to evaluate pneumonia versus COPD exacerbation. Diagnosis: shortness of breath (R06.02) pending workup.”
CMS audit pattern: Repeated R06.02 coding across consecutive visits with no documented progress toward a definitive diagnosis triggers Targeted Probe and Educate (TPE) review. Payers expect diagnostic closure. Use R06.02 past two or three visits, and the note has to document why the cause stays unconfirmed.
Outpatient vs Inpatient Documentation Rules for SOB
|
Setting |
Documentation status |
Correct code |
|---|---|---|
|
Outpatient |
“Shortness of breath” documented, no cause confirmed |
R06.02 (primary) |
|
Outpatient |
“Possible CHF with SOB,” not yet confirmed |
R06.02 only, since outpatient uncertain diagnoses aren't coded as confirmed |
|
Outpatient |
“SOB secondary to confirmed COPD exacerbation” |
J44.1 primary, R06.02 dropped as integral symptom |
|
Inpatient |
“Probable heart failure with dyspnea” |
I50.9 coded as confirmed per inpatient guidelines, R06.02 dropped |
|
Inpatient |
“Shortness of breath under evaluation” |
R06.02 as principal diagnosis pending workup |
|
Emergency department |
“r/o PE, r/o CHF, SOB” |
R06.02 plus objective findings such as R09.02 for documented hypoxemia, not the ruled-out conditions |
Per the ICD-10-CM Official Guidelines for Coding and Reporting (Updated April 1, 2026), outpatient uncertain diagnoses, including probable, suspected, or rule-out conditions, can't be coded as confirmed (ftp.cdc.gov).
The StatPearls dyspnea classification cited above is at ncbi.nlm.nih.gov/books/NBK499965/.
Documentation gaps on R06.02 claims are the leading cause of CO-16 denials and TPE audit selection across internal medicine and emergency medicine. MedSole RCM's pre-submission documentation review catches these gaps before the claim leaves the practice, at 2.99% of collections. Provider credentialing at $99 per payer makes sure the rendering provider is enrolled before the claim goes out.
CPT Codes That Pair With R06.02: What Survives Payer Review and What Gets Denied
The shortness of breath ICD-10 code never works a claim alone. Every CPT service billed next to it has to be justified by the diagnosis, and the diagnosis code has to be specific enough to support the procedure.
The CPT Codes Providers Bill Most Often With R06.02
|
CPT code |
Procedure |
Pairs with R06.02? |
Medical necessity threshold |
Payer consideration |
|---|---|---|---|---|
|
99213-99215 |
Office or outpatient E/M |
Yes, primary pairing |
Documented SOB with clinical decision-making; MDM level sets the visit level |
Higher-level visit holds when functional limitation is documented |
|
94760 |
Noninvasive pulse oximetry |
Yes |
Documented SOB with suspected hypoxia |
Bundled into same-day E/M; don't bill separately for routine monitoring |
|
71046 |
Chest X-ray, two views |
Yes |
Clinical indication: new-onset SOB, fever, or abnormal exam |
Medicare expects the indication in the note |
|
94010 |
Spirometry |
Yes, especially with R06.09 |
Pulmonary function evaluation for exertional or chronic dyspnea |
Note has to document why PFT was indicated |
|
93306 |
Echocardiography |
Yes, with cardiac context |
Cardiac cause evaluation with documented cardiac risk factors |
SOB alone without cardiac documentation can draw CO-50 |
|
94015 |
Patient-initiated spirometry |
Only with documented chronic SOB management |
Ongoing monitoring needing a prior diagnosis |
Not for initial R06.02 evaluation |
|
99000 |
Specimen handling |
No |
Not a diagnostic service for SOB |
Flagged here as an incorrect pairing seen in denial patterns |
Procedure-diagnosis alignment: CPT 93306 (echocardiography) billed with R06.02 and no documented cardiac indicators, no risk factors, no abnormal cardiac exam, no family history, draws a CO-50 medical necessity denial. The diagnosis has to justify the procedure. R06.02 alone won't support cardiac imaging.
The Medicare Coverage Rule for Diagnostic Testing on SOB
Medicare reviews R06.02 claims for diagnostic services closely, since symptom-only codes without workup progression raise necessity questions. Three expectations apply.
A clinical evaluation confirming SOB has to precede instrumental testing. Tests billed with no preceding evaluation that documents the indication draw CO-50 on the follow-on claims.
Multiple studies on the same date each need their own necessity documentation. “Shortness of breath” doesn't automatically justify a chest X-ray, ECG, echocardiogram, and PFT on one visit. Each needs its own clinical rationale.
Symptom codes on risk-adjusted claims affect quality metrics differently than confirmed diagnoses. Practices in value-based arrangements should watch persistent R06.02 coding without diagnostic progression, since it weakens risk-adjustment completeness.
Same-day multi-procedure rule: Billing several diagnostic studies with R06.02 on one date means documenting the rationale for each study separately. “Rule out multiple causes of SOB” doesn't cut it. Each study needs its own documented indication.
Medicare coverage for diagnostic services tied to respiratory symptom codes runs through the CMS Local Coverage Determination framework (cms.gov/medicare/coding-billing/icd-10-codes).
R06.02 Claim Denials: The Four Patterns That Trigger CO-16, CO-50, and OIG Audit Selection
A denied R06.02 claim tells you exactly where the documentation or coding broke down. The denial code on a shortness of breath ICD-10 claim points straight at the gap. Four patterns account for most SOB claim rejections across specialties.
The Four Denial Codes That Hit R06.02 Claims Most Often
|
Denial code |
Description |
Root cause in SOB claims |
Specific trigger |
Prevention |
Appeal |
|---|---|---|---|---|---|
|
CO-16 |
Claim lacks information |
Note doesn't state SOB as a confirmed symptom, or onset and context are missing |
SOB implied from vitals but not stated in the assessment |
Pre-submission checklist confirming SOB sits in the assessment with onset and context |
Resubmit with the full note; highlight the assessment entry |
|
CO-50 |
Not medically necessary |
Diagnostic CPT doesn't align with R06.02 specificity or clinical indicators |
Echo (93306) or spirometry (94010) billed with no documented indication |
Document the rationale for each diagnostic service before submission |
Appeal with records showing the indicators that justified each procedure |
|
CO-4 |
Service inconsistent with the code |
R06.09 was correct but R06.02 was submitted; the CPT needs exertional documentation |
Notes document “dyspnea on exertion” but the claim shows R06.02 |
Audit notes before code selection; code R06.09 when “exertional” appears |
Resubmit with R06.09 plus documentation of the exertional context |
|
Type 1 Excludes edit |
Automatic rejection for an incompatible combination |
R06.02 billed with J80, J96.x, or R09.2 |
Both codes on one claim trip an automatic edit |
Never combine R06.02 with excluded codes; use the higher-specificity code only |
Not appealable as a clinical decision; resubmit with one appropriate code |
CO-16 on R06.02 claims: When CO-16 recurs across providers in a practice, the problem is documentation workflow, not coding workflow. CO-16 means the claim lacks information, which for R06.02 almost always means the assessment has no explicit SOB language. Audit the note template, not the code.
CO-50 prevention: The fastest fix is documenting the rationale for each diagnostic service in its own sentence. Not “chest X-ray ordered.” Instead: “Chest X-ray ordered to evaluate infectious versus obstructive etiology of acute-onset SOB with 88% saturation on room air.”
OIG Audit Triggers Specific to SOB Coding
-
Using R06.02 across three or more consecutive visits for the same patient with no documented progress toward a diagnosis and no note explaining why the cause stays unconfirmed. Auditors and Medicare Administrative Contractors flag this static-symptom pattern for TPE review.
-
Billing advanced diagnostics (93306, 94010) repeatedly with R06.02 and no documented clinical progression between studies. Auditors look for a diagnostic sequence: initial evaluation, then targeted testing based on findings.
-
Copy-paste SOB documentation where the language is identical across visits. EHR auto-populated notes with the same shortness of breath text every visit are a primary OIG documentation flag in internal medicine and emergency medicine.
-
Billing R06.09 for a patient whose notes consistently document rest-onset SOB. Upcoding the specificity beyond what the notes support is a specific OIG target in cardiology and pulmonology billing.
The OIG Work Plan identifies symptom-code overuse, including repeated R06.02 coding without diagnostic progression, as a recurring source of Medicare improper payments (oig.hhs.gov/reports-and-publications/workplan).
Practices carrying a CO-16 or CO-50 backlog on R06.02 claims need a billing partner that reviews documentation before the claim leaves the office. MedSole RCM's medical billing services catch these patterns upstream, with a 99% clean claim rate on respiratory billing at 2.99% of collections.
When credentialing gaps drive CO-50 denials, provider credentialing at $99 per payer, the most affordable enrollment rate in the market, fixes the upstream problem before it becomes a downstream denial.
How Common Is Shortness of Breath? The 2025-2026 Clinical Data That Strengthens Every Medical Necessity Argument
Clinical burden data strengthens medical necessity arguments in prior authorization requests and CO-50 appeals. These are the current peer-reviewed figures.
Per UpToDate (literature review current through May 2026), dyspnea can present as the primary manifestation of lung disease, myocardial ischemia or dysfunction, anemia, neuromuscular disorders, obesity, or deconditioning. That clinical range spans every major specialty MedSole bills for. Dyspnea affects millions worldwide and serves as a leading reason for encounter across emergency medicine, internal medicine, cardiology, and pulmonology.
That multi-system reach is why the shortness of breath ICD-10 code shows up as a high-frequency code across specialties, and why coding accuracy and documentation specificity move revenue in internal medicine, emergency medicine, cardiology, and pulmonology at the same time.
Per NIH and NCBI StatPearls (Updated December 2025), dyspnea is a subjective respiratory sensation of insufficient air intake arising from physiologic, psychological, social, and environmental interactions. The subjective nature is exactly why documentation specificity is required. The provider has to translate a patient's subjective experience into objective clinical language that justifies R06.02 and the services billed with it.
Shortness of breath ranks among the top five chief complaints in U.S. emergency department visits each year, per MedlinePlus (NIH and NLM). High volume across specialties means small errors, using R06.02 when R06.09 is correct or omitting onset, add up to cumulative revenue leakage at scale.
Volume consequence: A practice submitting 200 SOB claims a month at a 15% documentation-gap denial rate, the industry average for symptom-only codes, loses about 30 claims a month to preventable denials. At an average R06.02 encounter value of $150, that's $4,500 a month in recoverable revenue that clean documentation and code selection would protect.
Post-stroke and elderly patients with aspiration risk present SOB alongside swallowing disorders; when both are separately documented, report the dysphagia ICD-10 code R13.10 with R06.02. Heart failure patients with concurrent sleep disruption may qualify for additional coding under insomnia ICD-10 code G47.00 for the cardiac co-coding workflow.
Dyspnea's multi-system significance is documented by UpToDate (literature review current through May 2026) and MedlinePlus (NIH and NLM) at medlineplus.gov/breathingproblems.html.
Frequently Asked Questions About Shortness of Breath ICD-10 Coding
What is the ICD-10 code for shortness of breath?
R06.02 is the ICD-10-CM code for shortness of breath (SOB). It's billable and specific, valid for HIPAA-covered transactions from October 1, 2025 through September 30, 2026 under the FY2026 code set. Use R06.02 when the provider documents shortness of breath without a confirmed underlying cause.
What causes shortness of breath?
Shortness of breath comes from respiratory conditions such as COPD, asthma, and pneumonia, and from cardiac conditions such as heart failure. The confirmed cause sets the primary ICD-10 code. R06.02 applies only when the provider hasn't established an underlying cause.
What does it mean if you are short of breath?
Shortness of breath, medically termed dyspnea, is a subjective sense of uncomfortable or difficult breathing. In billing, it codes to R06.02 when the provider documents the symptom without confirming a specific disease. Confirmed causes carry their own disease codes, not R06.02.
Is shortness of breath billable?
Yes. R06.02 is a billable ICD-10-CM code valid for HIPAA-covered claims. The parent code R06.0 is not billable. Submit the five-character R06.02 subcode every time, because R06.0 on its own draws an automated clearinghouse rejection.
What is the ICD-10 code for shortness of breath unspecified?
R06.02 is the ICD-10 code for shortness of breath unspecified, meaning general breathing difficulty with no specified type, pattern, or confirmed cause. R06.00 (dyspnea, unspecified) is related but distinct, used when the provider documents “dyspnea” rather than “shortness of breath.”
What is the ICD-10 code for shortness of breath on exertion?
Shortness of breath on exertion uses R06.09 (Other forms of dyspnea), not R06.02. R06.02 covers general, unspecified SOB. When the provider documents dyspnea on exertion or DOE, R06.09 is correct. Coding R06.02 for documented exertional dyspnea creates a documentation-to-code mismatch that draws payer denials.
What is the ICD-10 code for acute shortness of breath?
Acute-onset shortness of breath that doesn't meet criteria for acute respiratory distress uses R06.02. R06.03 (Acute respiratory distress) is reserved for presentations meeting clinical severity criteria. Document the onset timeline plainly, since “acute onset SOB for two days” supports the diagnostic workup billed.
What is the ICD-10 code for shortness of breath in pregnancy?
Shortness of breath in pregnancy with no confirmed cause uses R06.02 alongside Z34.x (supervision of pregnancy). If SOB stems from a confirmed pregnancy complication, code the O-series complication first. R06.02 fits physiologic dyspnea of pregnancy when no pathologic cause is documented.
What is the ICD-10 code for post-COVID shortness of breath?
Post-COVID shortness of breath uses a three-code protocol: U09.9 (Post-COVID-19 condition, unspecified) first, R06.02 second for the active respiratory symptom, and Z86.16 (Personal history of COVID-19) when prior confirmed COVID is documented. Don't use U07.1 (active COVID-19) for a residual post-COVID encounter.
What is the intercostal pain with shortness of breath ICD-10 code?
When intercostal pain accompanies shortness of breath with no confirmed cause, report both: R06.02 for the SOB and M54.6 or R07.81 for the chest pain, depending on the documentation. Each condition has to be separately documented and addressed. Use only the codes the provider's assessment supports.
The CDC ICD-10-CM Browser Tool confirms the current operative mapping for all R06.02 queries under the FY2026 April 1, 2026 release (icd10cmtool.cdc.gov).
Getting R06.02 Right the First Time: The Five-Element Pre-Submission Checklist
Getting the shortness of breath ICD-10 code right comes from five checks applied before the claim goes out, not corrections made after the denial lands.
The Pre-Submission Checks That Protect Every R06.02 Claim
-
Code accuracy. Confirm the provider's documented term. “Dyspnea on exertion” or “DOE” means R06.09 before submission. “Dyspnea lying flat” or “orthopnea” means R06.01. “Shortness of breath” with no qualifier means R06.02.
-
Documentation completeness. Confirm onset timeline, context, oxygen saturation, and clinical impression sit in the assessment. A complete note protects against CO-16. An incomplete one creates it.
-
CPT-to-diagnosis alignment. Verify each CPT links to R06.02 through the diagnosis pointer (Box 24E on the CMS-1500) and that the note carries a separate rationale for each diagnostic service. Misaligned pointers draw CO-4 denials.
-
Type 1 Excludes check. Confirm no excluded code (J80, J96.x, R09.2) sits on the same claim as R06.02. Those combinations trip automatic clearinghouse rejections before human review.
-
Credentialing verification. Confirm the rendering provider is enrolled with the billing payer before submission. A credentialing gap on a clean R06.02 claim draws CO-50 before the documentation is even read.
Pre-submission rule: An R06.02 claim that clears all five checks before it leaves the practice pays on process, not luck. Each item missed adds one more denial to the aging report.
How MedSole RCM Manages SOB Billing for Internal Medicine, Emergency Medicine, Cardiology, and Pulmonology
MedSole RCM manages the full revenue cycle for internal medicine, emergency medicine, cardiology, and pulmonology providers billing R06.02 and related respiratory encounters across Medicare, Medicaid, and commercial payers.
The billing fee is 2.99% of collections, the most affordable full-service medical billing rate available to internal medicine and emergency medicine providers in the market. No setup fees, no long-term contracts.
For practices that need enrollment before billing, MedSole RCM credentials internists, cardiologists, pulmonologists, and emergency medicine physicians at $99 per payer, the lowest per-payer credentialing fee in the market. A cardiology practice credentialing with 15 payers pays $1,485 total. Comparable credentialing runs $150 to $300 per payer elsewhere.
MedSole's clean claim rate on respiratory and SOB encounters is 99%. The billing team tracks ICD-10-CM updates, including mid-year releases like the April 1, 2026 update, so practices never submit R06.02 claims on outdated files that reject clinically correct encounters.
Internal medicine, emergency medicine, cardiology, and pulmonology practices can review the full offering on MedSole RCM's medical billing services page or explore revenue cycle management for cardiology and pulmonology for a complete RCM partnership.
R06.02 Code Decision Summary
-
Provider documents “shortness of breath” or “SOB” with no qualifier and no confirmed cause: use R06.02.
-
Provider documents “dyspnea on exertion,” “SOB with activity,” or “DOE” and no confirmed cause: use R06.09.
-
Provider documents “orthopnea” or “SOB lying flat” and no confirmed cause: use R06.01.
-
Provider confirms COPD, asthma, pneumonia, or heart failure as the cause: code the disease first and drop R06.02 as an integral symptom.
-
Patient has documented residual post-COVID SOB: use U09.9 first, R06.02 second, Z86.16 third.
-
Claim shows R06.02 with J80, J96.x, or R09.2: remove R06.02, since a Type 1 Excludes violation forces an automatic rejection.
Verify current code validity for FY2026 dates of service at the CDC ICD-10-CM Browser Tool, and check MedlinePlus for clinical context on SOB causes (icd10cmtool.cdc.gov and medlineplus.gov/breathingproblems.html).
Providers whose R06.02 billing fails any of the five pre-submission checks pay for those gaps in denied claims and delayed reimbursement. MedSole RCM closes them at 2.99% of collections. Provider credentialing runs $99 per payer, with no setup fees and no long-term contracts. Contact MedSole RCM for a no-obligation review of your respiratory encounter volume.

.webp)