![CPT Code 99204: Billing, Reimbursement & Documentation Guide [2026]](https://medsolercm.com/_imgs/blogs/92836_cpt-99204-billing-documentation-guide.webp)
![CPT Code 99204: Complete Billing, Reimbursement & Documentation Guide [2026]](/_imgs/blogs/92836_cpt-99204-billing-documentation-guide.webp)
Quick Facts: CPT Code 99204
Before diving into the full breakdown, here's a quick-reference snapshot of 99204. Bookmark this table for fast lookups during coding and claim submission.
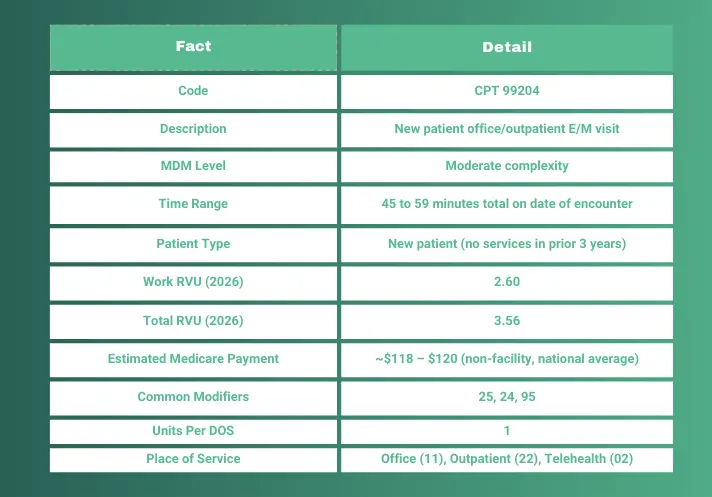
Each element above is covered in full detail throughout this guide, with documentation checklists, real SOAP note examples, payer-specific reimbursement rates, and step-by-step billing workflows.
CPT code 99204 is an evaluation and management (E/M) code used to report a new patient office or other outpatient visit requiring moderate medical decision-making (MDM) or 45 to 59 minutes of total time spent on the date of the encounter. It's one of the most commonly billed new patient codes in primary care, internal medicine, and specialty practices.
This guide breaks down everything you need to bill the 99204 CPT code correctly in 2026. You'll find current RVU values, Medicare and commercial reimbursement rates, documentation checklists, modifier rules, denial prevention strategies, and real clinical scenarios with ICD-10 pairings.
Every section reflects the latest CMS physician fee schedule updates, current AMA coding changes, and payer-specific billing requirements for 2026.
Whether you're a provider documenting a new patient office visit, a coder selecting the right E/M level, or a billing manager tracking denials, you'll find practical, audit-ready guidance you can put to work on your next claim.
What Is CPT Code 99204?
99204 CPT Code Description (Official AMA Definition)
The official 99204 CPT code description from the American Medical Association reads:
"Office or other outpatient visit for the evaluation and management of a new patient, which requires a medically appropriate history and/or examination and moderate level of medical decision making. When using total time on the date of the encounter for code selection, 45 minutes must be met or exceeded."
In plain terms, this CPT code 99204 definition covers a new patient visit where the clinical picture is complex enough to require moderate MDM. Think multiple chronic conditions, a new diagnosis with an uncertain prognosis, or starting a patient on prescription medications.
The AMA last verified this 99204 description on January 26, 2026. Their typical patient example describes "a new patient with a progressing illness or acute injury requiring medical management or possible surgical treatment."
The full CPT code 99204 description hasn't changed since the 2021 E/M restructuring, but knowing the exact language matters when you're defending documentation in an audit.
Here's what did change in 2021. Providers can now select 99204 based on either moderate MDM or total time of 45 to 59 minutes. You don't need to meet both. Pick whichever method your documentation supports, and make sure your note clearly backs up that choice.
Who Can Bill CPT Code 99204?
Any qualified provider who meets the documentation requirements can bill this code. That includes:
-
Physicians (MD/DO)
-
Nurse practitioners (NP)
-
Physician assistants (PA)
Can a physician assistant bill 99204? Yes, absolutely. Under Medicare, NPs and PAs are reimbursed at 85% of the physician fee schedule. That means the practice receives a lower payment when a non-physician provider bills the same code. But the code itself is available to all three provider types.
99204 has no age restrictions, covering newborns through geriatric patients. Specialty doesn't limit it either. Primary care, cardiology, psychiatry, dermatology, ophthalmology, and orthopedics all use this code for new patient encounters involving moderate complexity.
How Many Minutes Is CPT 99204? Time Requirements Explained
What Counts as Total Time for 99204?
The 99204 time requirement is 45 to 59 minutes of total time on the date of the encounter. Not face-to-face time. Total time.
That distinction matters. Under the current AMA E/M time guidelines, "total time" covers both face-to-face and non-face-to-face activities on the same calendar day. Here's what counts toward your CPT code 99204 time:
-
Reviewing patient history and external records
-
Performing the exam and clinical evaluation
-
Counseling and educating the patient or family
-
Ordering tests and referrals
-
Documenting clinical findings in the EHR
-
Coordinating care with other professionals
-
Interpreting results (when not separately reported)
And here's what doesn't count:
-
Administrative work unrelated to the patient's care
-
General research not specific to this patient
-
Teaching that isn't tied to the patient's condition
One common misconception: the midpoint rule doesn't apply to E/M level selection by time. You can't round up to 99204 if your time lands at 40 minutes. The time for 99204 must meet or exceed 45 minutes. Fall short by even a minute, and you're in 99203 territory.
Time Documentation Best Practices
If you're billing 99204 based on time, your note needs to say so. Clearly. A vague statement like "appropriate time spent" won't hold up in an audit, and it won't survive a payer review either.
Here's a template that works:
"Total time personally spent by me on the date of the encounter: [XX] minutes (includes chart review, patient evaluation, counseling, orders, documentation, and care coordination)."
Drop that line at the bottom of every time-based note. It takes five seconds and protects the entire claim.
Now, the flip side. If you're billing by MDM instead of time, there's no requirement to document time at all. Some providers include it anyway for completeness, but the 99204 time requirement only kicks in when time is your code selection method.
Medical Decision-Making (MDM) Requirements for CPT Code 99204
To bill CPT code 99204 based on MDM, the visit must involve moderate complexity medical decision-making. Moderate MDM requires meeting at least two of three elements at the moderate level: the number and complexity of problems addressed, the amount and complexity of data reviewed, and the risk of complications or morbidity.
That's the 99204 requirement: two out of three at moderate complexity. Let's break down each element for this level 4 E/M code.
Element 1: Number and Complexity of Problems Addressed
Moderate complexity here means the visit involves clinical problems that go beyond straightforward. Any of the following qualify:
-
One or more chronic illnesses with mild exacerbation or progression
-
Two or more stable chronic conditions being actively managed
-
An undiagnosed new problem with uncertain prognosis
-
An acute illness with systemic symptoms (fever plus respiratory distress, for example)
A single stable chronic condition managed without changes won't meet this threshold. The problems addressed during the visit need to carry real clinical weight.
Element 2: Amount and Complexity of Data Reviewed
For moderate data complexity, you need to show that clinical information was gathered, reviewed, or analyzed beyond a basic level. Qualifying activities include:
-
Reviewing prior external notes or records from another source
-
Ordering and reviewing diagnostic tests
-
Independent interpretation of a test (reading an in-office EKG yourself, for instance)
-
Discussion with an external physician or qualified health professional about management
Ordering a single basic lab panel without reviewing outside data won't typically reach moderate. The data element needs some depth to it.
Element 3: Risk of Complications, Morbidity, or Mortality
Moderate risk is where a lot of 99204 visits clearly qualify. Common moderate-risk scenarios include:
-
Prescription drug management (starting, adjusting, or continuing medications)
-
Decision for minor surgery with identified patient risk factors
-
Diagnosis or treatment significantly limited by social determinants of health
Starting a new prescription is the most common qualifier here. If the provider writes a new Rx during a new patient visit, that alone satisfies moderate risk.
The AAFP's "Outpatient E/M Coding Simplified" guide provides a helpful visual MDM table that maps all three elements side by side.
MDM vs. Time: Which Should You Choose?
Providers can bill the 99204 CPT code using either method. They don't need to meet both.
If the MDM is moderate but the visit only took 30 minutes, you can still bill 99204 using MDM-based selection. No minimum time threshold applies. And if the visit ran 48 minutes but moderate medical decision-making wasn't quite there, time-based billing still supports 99204.
What matters is documenting which method drove your code selection. A single line in the note makes a real difference.
MedSole RCM Insight: In our experience processing thousands of E/M claims, providers who clearly state their code selection basis, either MDM or time, in their documentation see roughly 23% fewer downcoding events. A simple line like "Code selected based on moderate MDM" eliminates ambiguity for coders, auditors, and payers alike.
99204 Documentation Requirements: Your Audit-Proof Checklist
Documentation is what separates a paid 99204 claim from a denied one. Your provider can deliver textbook moderate MDM, but if the note doesn't reflect that complexity clearly, the claim gets downcoded or kicked back. Here's what's required to bill 99204 and keep it audit-proof.
Documentation Checklist for MDM-Based Billing
Every 99204 CPT code claim backed by MDM should include these 10 elements:
-
Chief complaint and reason for visit
-
Detailed HPI covering location, quality, severity, duration, timing, context, modifying factors, and associated signs/symptoms
-
Review of systems across pertinent body systems
-
Past, family, and social history as clinically relevant
-
Comprehensive physical examination findings
-
Assessment showing problems addressed during this visit, not just a rehash of the problem list
-
Data explicitly reviewed or ordered, naming specific labs, imaging, or external records
-
Risk explicitly stated: new prescription, surgical decision, or social determinant limitation
-
Plan with treatment decisions, follow-up instructions, and referrals
-
Provider signature and date
Items 6, 7, and 8 are where most notes fall apart. Auditors aren't scanning for a diagnosis list. They want to see which problems the provider actively worked on, what data was personally reviewed or ordered, and what risk shaped those clinical decisions.
Documentation Checklist for Time-Based Billing
Billing by time instead of MDM? All 10 elements above still apply. Add two more:
-
Total time stated explicitly (or start and stop times)
-
Activities performed during that time
Without documented time, there's no foundation for time-based code selection. The clinical note can be flawless, but one missing time statement gives the payer grounds to deny.
99204 SOAP Note Example (Redacted)
Here's a sample note that meets CPT code 99204 documentation standards for both MDM and time. Use it as a structural reference, not a copy-paste template.
text
SUBJECTIVE: 58-year-old female presents as a new patient
with a 6-month history of progressive fatigue, unintentional
weight loss (12 lbs), and intermittent palpitations. No prior
workup performed. PMH: hypertension (untreated x2 years).
No current medications. Family hx: thyroid disease (mother).
Non-smoker.
OBJECTIVE:
VS: BP 142/88, HR 92, Temp 98.4, BMI 24.1
General: Fatigued appearance, no acute distress
HEENT: No thyromegaly, no lymphadenopathy
CV: Irregular rate, no murmurs
Lungs: Clear bilaterally
Abdomen: Soft, non-tender, no masses
Neuro: Alert, oriented, no focal deficits
ASSESSMENT:
1. Unintentional weight loss - R63.4
(new problem, uncertain prognosis)
2. Palpitations - R00.2
(new problem, requires workup)
3. Hypertension, uncontrolled - I10
(chronic, mild exacerbation)
PLAN:
- CBC, CMP, TSH, free T4 ordered
- EKG performed and independently interpreted in office
(irregular rhythm, no ST changes)
- Started lisinopril 10mg daily
- Referral to cardiology for palpitation workup
- Dietary counseling provided
- Return in 4 weeks for lab review
MDM SUMMARY: Moderate. Multiple new problems with uncertain
prognosis. Moderate data review (independent EKG interpretation,
lab orders, reviewed prior records from outside provider).
Moderate risk (new prescription drug management).
Code selected based on MDM.
TOTAL TIME: 52 minutes (chart review, evaluation, counseling,
orders, documentation, care coordination).
Look at what this note does right. Every MDM element gets called out by name. The assessment labels each problem as new or chronic and tags its clinical status. Data is specific: "independent EKG interpretation," not just "tests ordered." Risk ties directly to starting a new prescription.
That MDM summary at the end is technically optional. In practice, it's worth its weight in gold. It tells the auditor exactly why 99204 is justified without forcing them to reconstruct the logic from scattered sections of the note.
Billing Guidelines for CPT Code 99204
Clean claims start with a clean process. Billing code 99204 isn't just about selecting the right E/M level; it's about nailing every step before the claim goes out the door.
Step-by-Step Billing Workflow
-
Verify the patient qualifies as "new." No professional services from the same physician, or same specialty in the same group, within the prior three years.
-
Provider completes the visit and documents either MDM level or total time.
-
Coder reviews the note and selects 99204 based on documented support, not the provider's superbill checkbox.
-
Pair with appropriate ICD-10 codes that justify medical necessity for a moderate-complexity encounter.
-
Assign the correct Place of Service code.
-
Apply modifiers if needed (25 for same-day procedure, 24 for post-op period, 95 for telehealth).
-
Submit the clean claim with all required fields populated.
-
Monitor for denials and respond within the payer's appeal window, typically 90 to 180 days.
Step 3 deserves extra attention. The coder's job is to match the code to documentation, not to the provider's preference. If the note supports 99203, that's what gets billed, regardless of what the superbill says.
To ensure clean claim submission and avoid costly coding errors, many practices partner with an outsourced medical billing team that specializes in E/M coding accuracy.
Common ICD-10 Codes Paired with 99204
These diagnosis codes show up most often alongside medical billing code 99204:
|
ICD-10 Code |
Description |
Typical Scenario |
|
E11.65 |
Type 2 diabetes with hyperglycemia |
New patient with uncontrolled diabetes |
|
I10 |
Essential hypertension |
New patient with elevated blood pressure |
|
I48.91 |
Unspecified atrial fibrillation |
New cardiac arrhythmia workup |
|
F32.9 |
Major depressive disorder, unspecified |
New mental health evaluation |
|
R63.4 |
Abnormal weight loss |
Unexplained weight loss workup |
|
M54.5 |
Low back pain |
New referral for chronic back pain |
|
J06.9 |
Acute upper respiratory infection |
Complex URI in a new patient |
Here's something to watch for: your ICD-10 selection needs to match the complexity you're claiming. A CPT code 99204 paired with only J06.9 will likely trigger a payer review. The diagnosis should justify moderate MDM or 45-plus minutes of provider time.
For current guidelines, CMS maintains an updated ICD-10 coding reference on their website.
Place of Service (POS) Codes for 99204
Your POS code tells the payer where the encounter happened. It also directly affects how much you get paid:
-
POS 11 (Office): Most common setting, highest physician payment
-
POS 22 (On-campus outpatient hospital): Lower physician payment since the facility bills separately
-
POS 02 (Telehealth, not patient's home): Real-time audio/video encounter
-
POS 10 (Telehealth, patient's home): Same format as POS 02, patient located at home
Getting the POS wrong doesn't just cause a denial. It can trigger an overpayment recoupment months later if a payer audits and finds you billed non-facility rates for a facility-based encounter. That's money you'll have to send back.
Does CPT Code 99204 Need a Modifier? When and How to Use Them
CPT code 99204 doesn't always require a modifier. But modifier 25 is commonly appended when a separately identifiable E/M service is performed on the same day as a procedure. Modifier 24 applies during a postoperative global period, and modifier 95 indicates a synchronous telehealth encounter.
Modifier 25: Significant, Separately Identifiable E/M
Modifier 25 is the most common modifier paired with CPT code 99204. Append it when the provider performs both a new patient E/M visit and a procedure on the same date of service. A typical scenario: new patient evaluation for a suspicious skin lesion, plus excision of that lesion.
Here's the thing: the E/M documentation needs to stand on its own. The note must show that the evaluation was clearly separate from the work already bundled into the procedure. Payers look for distinct ICD-10 codes supporting each service. One shared diagnosis between both claims almost guarantees a denial.
2026 G2211 update: G2211 is only payable alongside modifier 25 when the procedure is a Part B preventive service, immunization, or annual wellness visit. Pair G2211 with modifier 25 on any other procedure type, and the add-on code gets denied.
Modifier 24: Unrelated E/M During a Postoperative Period
Modifier 24 tells the payer this new patient visit is unrelated to a surgery another provider performed. Use it when the encounter falls within that surgeon's global period but addresses a completely different clinical problem.
Link the claim to a separate diagnosis code, and document why the visit has nothing to do with the surgical recovery. Without that distinction, the payer assumes it's part of the surgical follow-up and denies the E/M outright.
Picture a cardiologist seeing a new patient for atrial fibrillation while that patient is still in a 90-day global from a knee replacement. That's a textbook modifier 24 scenario.
Modifier 95: Synchronous Telehealth
Append modifier 95 when the entire 99204 encounter takes place through real-time audio and video. Phone-only calls don't qualify for this modifier.
Three documentation elements matter here: patient consent for telehealth, the platform used, and confirmation that MDM or time requirements were fully met during the synchronous session. Match the modifier with POS 02 (telehealth, not patient's home) or POS 10 (telehealth, patient's home) on the claim form.
Some commercial payers require different telehealth modifiers or place-of-service reporting. Verify your contracts before billing.
For detailed modifier application rules, the AAPC's modifier reference guidelines are worth reviewing.
Struggling with modifier denials on your E/M claims? MedSole RCM's certified billing team handles complex coding at just 2.99% of collections, the most affordable full-service billing in the market. Explore Our Medical Billing Services →
99204 CPT Code Reimbursement Rates & RVU Values (2026)
Medicare reimbursement for CPT code 99204 averages approximately $118 to $120 nationally for non-facility settings in 2026. That estimate is based on a total RVU of 3.56 and the CY 2026 conversion factor of $33.40. Commercial payers typically reimburse at 120% to 250% of Medicare rates, with allowed amounts ranging from $150 to $300 depending on contract and region.
Yes, CPT code 99204 is covered by Medicare. It's a standard E/M code on the physician fee schedule with no special coverage restrictions.
99204 RVU Breakdown (2026)
The RVU for 99204 breaks down into three components:
|
RVU Component |
Value |
|
Work RVU (wRVU) |
2.60 |
|
Practice Expense RVU (PE) |
0.76 (non-facility estimate) |
|
Malpractice RVU (MP) |
0.20 (estimate) |
|
Total RVU |
3.56 |
The 99204 wRVU of 2.60 reflects the physician's cognitive work and clinical effort. Practice expense covers overhead costs like staff, equipment, and supplies. Malpractice accounts for professional liability.
Medicare Reimbursement for 99204
For CY 2026, CMS established two separate conversion factors for the first time under the Medicare Physician Fee Schedule final rule:
-
QP (qualifying APM participants): $33.5675
-
Non-QP providers: $33.4009
For non-QP providers in a non-facility setting, the national estimate works out to 3.56 × $33.40, or roughly $118.90. Your actual 99204 reimbursement will vary based on where you practice, since CMS adjusts payments through Geographic Practice Cost Indices (GPCI).
Worth noting: 99204 is exempt from the 2026 efficiency adjustment, a 2.5% reduction that applies to certain other services.
To check your exact locality rate, use the CMS Physician Fee Schedule Lookup Tool.
Commercial Payer Reimbursement Rates
How much does insurance pay for 99204 beyond Medicare? That depends on your contracted rates. Here are approximate national averages:
|
Payer |
Average Allowed Amount |
|
Medicare |
~$118 – $120 |
|
UnitedHealthcare |
~$182 |
|
Blue Cross Blue Shield |
~$182 |
|
Aetna |
~$176 |
|
Cigna |
~$245 |
|
Commercial Average |
~$160 – $300 |
(Source: PayerPrice.com national average data, 2026)
These numbers shift based on your contract terms, geographic market, and network tier. A 99204 CPT code cost in Manhattan won't look anything like one in rural Kansas.
Facility vs. Non-Facility Rates
Non-facility rates (office, POS 11) pay more because the practice absorbs all overhead. Facility rates (hospital outpatient, POS 22) pay the physician less because the hospital bills separately for its own resources.
For 99204, non-facility payments typically run $30 to $50 higher. Billing the wrong POS code means you'll either leave money on the table or face a recoupment months later.
G2211 Add-On Code: Extra Revenue per Encounter
G2211 can add approximately $16 to $19 to your Medicare payment on qualifying 99204 visits. Report it when the billing provider serves as the continuing focal point for a patient's ongoing condition or complex illness.
New for 2026: G2211 is also reportable with home and residence E/M codes (99341 through 99350). Here's the restriction: you can't bill G2211 with modifier 25 unless the paired procedure is a Part B preventive service, immunization, or annual wellness visit.
Optimizing reimbursement on codes like 99204 requires a solid revenue cycle management process.
99203 vs 99204 vs 99205: Which New Patient Code Should You Use?
The key difference between these new patient CPT codes comes down to medical decision-making complexity and time. 99203 requires low MDM and 30 to 44 minutes. 99204 requires moderate MDM and 45 to 59 minutes. 99205 requires high MDM and 60 to 74 minutes. Higher complexity yields higher reimbursement but demands stronger documentation.
Here's how they stack up side by side:
|
Element |
99203 |
99204 |
99205 |
|
Patient Type |
New |
New |
New |
|
MDM Level |
Low |
Moderate |
High |
|
Time Range |
30 to 44 min |
45 to 59 min |
60 to 74 min |
|
Work RVU (2026) |
1.60 |
2.60 |
3.50 |
|
Estimated Medicare Rate |
~$105 |
~$119 |
~$157 |
|
Typical Scenario |
Controlled HTN, minor complaint |
Multiple chronic conditions, Rx management |
Cancer diagnosis, complex psych evaluation |
o when do you pick each code?
99203 fits visits involving a single straightforward problem with limited workup. A new patient with well-controlled hypertension needing a refill and routine labs is a clean 99203.
99204 applies when the provider addresses multiple diagnoses, starts new prescriptions, or reviews moderate amounts of data. Think of a new patient presenting with uncontrolled diabetes plus hypertension, where medication changes and lab interpretation drive the clinical decisions.
99205 belongs to visits involving high-risk decisions, life-threatening conditions, or coordination across multiple specialists. A new cancer workup or a complex psychiatric evaluation with suicidal ideation and comorbidities lands here.
The difference between 99203 and 99204 is where we see the most revenue left behind.
🔎 MedSole RCM Insight: We frequently see practices defaulting to 99203 when 99204 is clinically justified, leaving approximately $52 per encounter on the table. Over 200 new patients per year, that's $10,400 in lost revenue. Accurate code selection starts with documentation training, not guesswork at the superbill.
For a complete breakdown of the lower-level code, read our CPT Code 99203: Billing, Reimbursement & Documentation Guide.
99204 vs 99214: New Patient vs. Established Patient
CPT codes 99204 and 99214 both represent level 4 office visits with moderate MDM, but the difference is patient status. 99204 is exclusively for new patients who haven't been seen in three or more years. 99214 covers established patients. Medicare reimburses 99204 at roughly $52 more per encounter because new patient visits require more comprehensive evaluation and documentation.
|
Element |
99204 (New) |
99214 (Established) |
|
Patient Type |
New (3-year rule) |
Established |
|
MDM |
Moderate |
Moderate |
|
Time |
45 to 59 min |
30 to 39 min |
|
Documentation |
More comprehensive |
Can be more focused |
|
Estimated Medicare Rate |
~$119 |
~$95 |
The clinical complexity is the same. What changes is the depth of history gathering, the time investment, and the reimbursement that follows.
The 3-Year Rule for New vs. Established Patients
A patient qualifies as "new" when they haven't received any professional services from the same physician, or same specialty within the same group, in the prior three years. Medicare narrows this further to face-to-face encounters specifically.
Group structure matters here. In a single-specialty group, every provider of that specialty shares new patient status. If Dr. Smith (internal medicine) saw the patient two years ago, Dr. Jones (also internal medicine, same group) can't bill the return visit as new. In a multi-specialty group, each specialty operates independently for the three-year clock.
Here's a practical tip that saves headaches: build the new patient verification into your scheduling and registration workflow, not your coding process. By the time the coder touches the claim, the visit is already done. If someone at the front desk had flagged the patient as established, the provider could have adjusted documentation accordingly. Catching it after the fact creates rework and billing delays.
99204 vs 99244: Office Visit vs. Consultation Code
CMS stopped paying for outpatient consultation codes (99241 through 99245) back in 2010. If your practice previously billed 99244 for specialist consultations on new patients, the correct replacement under Medicare is 99204 when moderate MDM is documented.
The old consultation framework required three specific elements: a requesting provider, a reason for the consultation, and a written report sent back to that requesting provider. Those documentation standards no longer drive code selection for Medicare claims.
Here's where it gets tricky. Some commercial payers still recognize and reimburse consultation codes. Aetna, for example, has historically accepted 99241 through 99245 on commercial plans. So has Cigna in certain markets. Before defaulting to 99204 across all payers, check your individual contracts.
When you're billing Medicare or any payer that follows CMS guidelines, use the standard E/M code. For a new patient visit with moderate MDM, that's CPT code 99204. For established patients in the same scenario, it's 99214. Don't overthink it.
The safest approach: bill the appropriate new or established patient E/M code unless you've confirmed in writing that the specific payer accepts consultation codes and reimburses them at a higher rate.
Not sure if your team is selecting the right E/M level for new patients? MedSole RCM's coding specialists reduce downcoding errors and maximize your collections, all at just 2.99% of collections. Request a Free Billing Audit →
Clinical Scenarios: When to Use CPT Code 99204 (with ICD-10 Codes)
Knowing the rules for CPT code 99204 is one thing. Seeing what constitutes a 99204 visit in practice is another. These four scenarios show exactly when 99204 is justified, with the MDM reasoning and ICD-10 codes you'd use on the claim.
Scenario 1: New-Onset Atrial Fibrillation
Patient: 67-year-old male, new patient, presenting with palpitations and episodic dizziness over the past three weeks.
Provider actions: Comprehensive cardiovascular history and exam. EKG performed and independently interpreted in office showing irregular rhythm. CHA₂DS₂-VASc score calculated. Anticoagulation initiated with apixaban. Cardiology referral placed for further evaluation.
ICD-10: I48.91 (Unspecified atrial fibrillation)
Why 99204: Moderate MDM. New problem with systemic symptoms satisfies element one. Independent EKG interpretation plus external record review covers moderate data. Starting anticoagulation meets moderate risk. Total time: 48 minutes.
Scenario 2: Uncontrolled Type 2 Diabetes with Hyperglycemia
Patient: 55-year-old female, referred from urgent care after a random glucose of 340 mg/dL. No established PCP.
Provider actions: Reviewed A1c (10.2%) and BMP from urgent care. Comprehensive metabolic assessment and foot exam completed. Initiated basal insulin with dosing instructions. Referred to dietitian. Ordered follow-up labs for four weeks.
ICD-10: E11.65 (Type 2 diabetes mellitus with hyperglycemia)
Why 99204: Moderate MDM. Chronic illness with exacerbation meets element one. Review of external lab data satisfies moderate data. Insulin initiation qualifies as prescription drug management under moderate risk. Total time: 51 minutes.
Scenario 3: Persistent Headaches with Neurological Workup
Patient: 42-year-old male, new patient, reporting daily headaches for three months unresponsive to OTC treatment.
Provider actions: Detailed neurological exam, all cranial nerves assessed. Brain MRI ordered to rule out structural pathology. Started sumatriptan trial for suspected migraines. Neurology referral if no improvement in six weeks.
ICD-10: R51.9 (Headache, unspecified)
Why 99204: Moderate MDM. New problem with uncertain prognosis checks element one. MRI order and review of prior outside records meet moderate data. New prescription satisfies moderate risk. Total time: 46 minutes.
Scenario 4: New Patient Depression with Medication Management
Patient: 38-year-old female, self-referred for worsening depression and anxiety over the past four months.
Provider actions: Comprehensive psychiatric history including trauma screening. PHQ-9 score: 16 (moderately severe). GAD-7 score: 14. Started sertraline 50mg daily. Safety plan discussed and documented. Therapy referral placed. Thyroid panel ordered to rule out medical causes.
ICD-10: F32.1 (Major depressive disorder, single episode, moderate)
Why 99204: Moderate MDM. New problem requiring workup satisfies element one. Standardized screening tools plus lab orders cover moderate data. SSRI initiation meets moderate risk. Total time: 53 minutes.
Each of these 99204 CPT code examples follows the same pattern: the visit addresses a clinical problem that goes beyond straightforward, the provider reviews or generates meaningful data, and the treatment plan carries real risk. If your encounters look like these, your documentation should reflect that complexity clearly enough for any auditor to follow.
Top Reasons 99204 Claims Get Denied, and How to Fix Them
Denials on 99204 CPT code claims follow predictable patterns. Once you know where the weak spots are, most of these are preventable with small workflow changes.
1. Insufficient MDM Documentation
The problem: The note shows clinical work happened, but it doesn't clearly demonstrate moderate complexity across two of three MDM elements. Auditors can't infer what's not written down.
The fix: Explicitly document problems addressed (not just listed), data personally reviewed or ordered by name, and the risk factor driving treatment decisions. A brief MDM summary at the end of the note eliminates guesswork.
2. Bundled with a Same-Day Procedure
The problem: The E/M gets denied because it was billed alongside a procedure without modifier 25, or the documentation doesn't show the E/M as distinct from the procedure's built-in pre and post work.
The fix: Document the E/M component as clearly separate from procedural work. Use distinct ICD-10 codes for each service. Append modifier 25 only when the evaluation genuinely stands on its own.
3. Patient Doesn't Qualify as "New"
The problem: The patient was seen by another provider of the same specialty within the same group in the prior three years. The claim gets kicked back as an established patient visit.
The fix: Verify new patient status at scheduling, not at coding. Build the three-year check into your registration workflow so the front desk flags it before the provider even walks in the room.
4. Time Documentation Errors
The problem: The provider billed by time but documented it vaguely, or the stated time falls outside the 45 to 59 minute window for 99204.
The fix: Use an explicit total time statement or start/stop times. "Approximately 45 minutes" won't survive a payer review. "Total time: 47 minutes" will.
5. Downcoded by Payer (Cigna Alert)
The problem: Cigna's policy effective October 1, 2025 allows automatic adjustment of 99204 and 99205 claims down one level when the payer determines the encounter criteria don't support the billed code.
The fix: Ensure every note explicitly supports each MDM element at the moderate level. With Cigna, vague documentation isn't just a denial risk; it's a guaranteed downcode.
How to Appeal a 99204 Denial
When a 99204 denial hits your AR, don't let it age. Follow this process:
-
Review the denial reason code (CO-4, CO-97, and CO-16 are common culprits)
-
Pull the original note and compare it against MDM or time requirements
-
Write the appeal letter citing specific documentation that supports 99204
-
Include relevant AMA CPT guidelines and the applicable MDM framework
-
Submit within the payer's appeal window, typically 90 to 180 days
Waiting past the appeal deadline means that revenue is gone permanently. No exceptions.
🔎 MedSole RCM Insight: Our denial management team has recovered over $2.3M in wrongfully denied E/M claims for our clients in 2025 alone. The most common pattern we see? Providers who document the right level of care but use language that doesn't map to payer audit criteria. A 10-minute documentation template adjustment can prevent thousands in lost revenue.
Learn how our denial management specialists recover lost revenue with a 98.5% clean claim rate. And our AR follow-up process ensures no 99204 denial goes unaddressed.
Can You Bill 99204 for Telehealth?
Yes, CPT code 99204 can be billed for telehealth encounters when the visit meets all standard requirements for MDM or time. Use modifier 95 for synchronous audio-video encounters and the appropriate Place of Service code: POS 02 or POS 10.
Phone-only visits don't qualify. The encounter must happen through real-time, two-way audio and video.
Telehealth Modifiers and POS Codes
Getting the modifier and POS combination right is the difference between a clean payment and a denial. Here's how to pair them:
-
Modifier 95: Synchronous telehealth, real-time audio and video
-
POS 02: Patient is located somewhere other than their home (clinic, office, facility)
-
POS 10: Patient is at home during the encounter
Your note needs to capture three things beyond the standard MDM or time documentation: patient consent for the telehealth visit, the platform used (Zoom, Doxy.me, integrated EHR video, etc.), and confirmation that the encounter was conducted via live audio-video.
Some commercial payers have their own telehealth modifier requirements that differ from Medicare. Check your contracts before assuming modifier 95 and POS 02 are universal.
DEA Telemedicine Prescribing Extension (Through December 2026)
HHS and the DEA extended telemedicine prescribing flexibilities through December 31, 2026. Providers can prescribe controlled substances via telehealth without requiring a prior in-person evaluation.
That's a big deal for new patient intakes. CPT 99204 visits involving pain management, ADHD medications, or anxiety prescriptions can happen entirely by video without the old in-person visit requirement. For practices building virtual new patient workflows, this extension keeps the door open through the end of 2026.
CMS also permanently adopted virtual presence for direct supervision, meaning the supervising physician can be present via real-time audio and video rather than physically on-site. You can review the latest Medicare telehealth policies on the CMS Telehealth hub.
🔎 MedSole RCM Insight: Navigating telehealth billing rules for codes like 99204 doesn't have to be complicated. Our team handles telehealth E/M coding, modifier application, and payer-specific compliance, all at just 2.99% of collections. We also offer provider enrollment and credentialing services at $99 per payer, the fastest and most affordable in the industry. Get Started →
2026 Updates Affecting CPT Code 99204
Several changes in the CY 2026 Medicare Physician Fee Schedule directly affect how you bill, get paid for, and document the 99204 CPT code. Here's what to adjust in your workflows right now.
CY 2026 Dual Conversion Factors
For the first time, CMS is using two separate conversion factors under the CY 2026 MPFS Final Rule:
-
Qualifying APM Participants (QP): $33.5675
-
Non-QP providers: $33.4009
This split comes from the One Big Beautiful Bill Act (H.R.1) and represents a 3.26% to 3.77% increase over CY 2025. The practical impact: you need to know whether each billing clinician qualifies as a QP when you're modeling revenue projections and fee schedule analysis.
A small difference per claim, but across hundreds of 99204 encounters per year, it adds up.
G2211 + Modifier 25: Updated Billing Rules
The G2211 add-on code rules that took effect January 1, 2025 carry forward into 2026 with one expansion. G2211 is now also reportable with home and residence E/M codes (99341 through 99350), not just office visit codes.
Here's the restriction that trips people up: G2211 is only payable alongside modifier 25 when the paired procedure is a Part B preventive service, immunization, or annual wellness visit. Bill G2211 with modifier 25 on any other same-day procedure, and it gets denied.
Revenue impact per qualifying encounter: approximately $16 to $19 from Medicare.
Cigna Downcoding Policy for 99204 and 99205
Effective October 1, 2025 and continuing into 2026, Cigna may automatically adjust 99204 and 99205 claims down one level when the payer determines encounter criteria don't support the billed code.
This isn't a manual audit. It's algorithmic. If your documentation is vague on any MDM element, Cigna's system can downcode 99204 to 99203 before a human even reviews the claim. Make sure every note explicitly supports moderate MDM across at least two of three elements.
CMS Prior Authorization Rule (January 2026)
Starting January 2026, payers regulated by CMS must respond to prior authorization requests through an electronic API rather than fax or phone. The goal is faster turnaround and fewer PA-related denials for services like E/M visits.
For practices, the change means your billing software or clearinghouse needs API-enabled PA workflows. Without that integration, you risk compliance gaps and slower authorization processing compared to practices that have already adopted the electronic format.
99204 by Specialty: Primary Care, Ophthalmology & Dermatology
How 99204 gets used varies by specialty. Here's what to watch for in the most common settings.
Primary care and family medicine is where 99204 shows up most often. New patient establish-care visits with multiple chronic conditions, medication starts, and lab orders typically land squarely at moderate MDM. Don't default to 99203 when the documentation supports 99204. That's money walking out the door.
Ophthalmology and optometry can bill 99204 for medical new patient visits, not refractive ones. A new glaucoma patient requiring prescription eye drop management meets moderate risk. But a visit focused solely on glasses or contact lens fitting doesn't qualify for E/M coding at all. Keep medical and refractive services clearly separated.
Dermatology practices commonly use 99204 when a new patient presents with multiple skin conditions requiring biopsy decisions. Modifier 25 comes into play frequently here since the E/M and the biopsy often happen on the same day. Document them as distinct services.
Psychiatry and mental health providers use 99204 for moderate-complexity new patient intakes where medication management begins. A comprehensive psychiatric evaluation with a new SSRI prescription and safety planning fits cleanly.
Can urgent care bill 99204? Technically yes, if the patient qualifies as new and the documentation supports moderate MDM. In practice, most urgent care encounters don't reach that complexity level.
One more question that comes up: is 99204 a preventive CPT code? No. It's a problem-oriented E/M code. Preventive visits use the 99381 through 99397 series.
Frequently Asked Questions About CPT Code 99204
1. What is CPT code 99204?
CPT code 99204 is an evaluation and management code for a new patient office or outpatient visit requiring moderate medical decision-making or 45 to 59 minutes of total provider time on the date of the encounter. It applies to patients not seen by the same provider or same specialty within the same group in the prior three years.
2. How many minutes is CPT 99204?
CPT 99204 requires 45 to 59 minutes of total time on the date of the encounter. Total time includes both face-to-face and non-face-to-face activities like chart review, documentation, care coordination, and counseling. If you're billing by time rather than MDM, you must document the total minutes explicitly in the note.
3. What is the difference between 99203 and 99204?
The main difference is complexity. 99203 requires low MDM and 30 to 44 minutes, while 99204 requires moderate MDM and 45 to 59 minutes. Medicare reimburses 99204 roughly $14 more than 99203. Choose 99204 when multiple diagnoses are addressed, new prescriptions are started, or moderate data is reviewed during the visit.
4. What is the difference between 99204 and 99214?
Both codes require moderate MDM, but 99204 is for new patients and 99214 is for established patients. 99204 requires 45 to 59 minutes versus 30 to 39 minutes for 99214. Medicare pays approximately $52 more for 99204 because new patient visits demand more comprehensive history gathering and evaluation.
5. How much does Medicare pay for CPT 99204?
Medicare reimburses approximately $118 to $120 for CPT 99204 in non-facility settings based on the 2026 national average. Actual payment varies by geographic location through GPCI adjustments. Commercial payers typically pay 120% to 250% of Medicare rates, with allowed amounts ranging from roughly $160 to $300 depending on the contract.
6. What is the RVU for 99204?
The total RVU for 99204 in 2026 is 3.56. That breaks down into a work RVU of 2.60, a practice expense RVU of approximately 0.76 (non-facility), and a malpractice RVU of roughly 0.20. Multiply the total RVU by the CMS conversion factor of $33.40 to estimate the Medicare allowed amount.
7. Does CPT code 99204 need a modifier?
Not always. Modifier 25 is required when a separately identifiable E/M service is performed on the same day as a procedure. Modifier 24 applies when the visit is unrelated to another provider's postoperative global period. Modifier 95 is used for synchronous telehealth encounters. Without a same-day procedure or special circumstance, no modifier is needed.
8. What documentation is needed for 99204?
Documentation must support moderate MDM across at least two of three elements: problems addressed, data reviewed, and risk. The note should include a chief complaint, detailed HPI, relevant ROS, exam findings, a clear assessment with active problems, named data sources, risk factors, and a treatment plan. If billing by time, total minutes must be explicitly stated.
9. Can a physician assistant bill 99204?
Yes. Physician assistants and nurse practitioners can bill 99204 when their documentation supports moderate MDM or 45 to 59 minutes of total time. Under Medicare, PA and NP services are reimbursed at 85% of the physician fee schedule rate. The documentation requirements are identical regardless of provider type.
10. Is CPT code 99204 covered by Medicare?
Yes, 99204 is a standard E/M code on the Medicare Physician Fee Schedule with no special coverage restrictions or prior authorization requirements. It's covered for all specialties and all patient ages when documentation supports moderate MDM or the required time threshold. Medical necessity must be established through appropriate ICD-10 diagnosis coding.
11. How often can you bill 99204?
You can bill 99204 once per new patient per date of service. Since it's exclusively a new patient code, the same provider or same specialty within the same group can only use it once for a given patient. After the initial visit, subsequent encounters use established patient codes (99211 through 99215).
12. Can you bill 99204 for telehealth?
Yes. CPT 99204 is billable for telehealth when the visit is conducted via synchronous, real-time audio and video and meets all standard MDM or time requirements. Append modifier 95 and use POS 02 (patient not at home) or POS 10 (patient at home). Phone-only encounters don't qualify.
13. What is the 3-year rule for new patients?
A patient qualifies as "new" when they haven't received any professional services from the same physician, or same specialty within the same group practice, in the prior three years. Medicare specifically limits this to face-to-face encounters. In single-specialty groups, all providers of that specialty share the same three-year clock for new patient status.
14. Is 99204 a preventive code?
No. CPT 99204 is a problem-oriented evaluation and management code, not a preventive service. It's used when the visit addresses specific medical complaints, diagnoses, or conditions requiring clinical decision-making. Preventive and wellness visits are reported using the 99381 through 99397 code series or the Medicare Annual Wellness Visit codes (G0438, G0439).
15. What are common denial reasons for 99204?
The most frequent denial triggers include insufficient MDM documentation that doesn't clearly show moderate complexity, bundling errors when billed same-day with a procedure without modifier 25, incorrect new patient status when the patient was seen within three years, and vague time documentation. Cigna's 2025 downcoding policy also auto-adjusts 99204 claims when criteria appear unsupported.
Maximize Your 99204 Reimbursement with Confidence
CPT code 99204 is one of the highest-value new patient codes your practice can bill, but only when documentation, coding, and claim submission all align. Moderate MDM or 45 to 59 minutes of total time gets you there. Clean documentation keeps you there.
With 2026 bringing dual conversion factors, expanded G2211 opportunities, and heightened payer scrutiny from Cigna's downcoding policy, accuracy matters more than it did last year. Every undercoded 99204 that defaults to 99203 costs your practice roughly $52 per encounter. Over a year, that adds up fast.
For practices seeking affordable, expert billing support, MedSole RCM offers full-service medical billing at 2.99% of collections, among the lowest rates in the industry, with provider enrollment and credentialing starting at just $99 per payer. Our certified coding team specializes in E/M optimization, denial prevention, and compliance with the latest CMS guidelines.
Ready to stop leaving money on the table?
MedSole RCM handles your medical billing at just 2.99% and credentialing at $99/payer, the fastest and most affordable in the market.
Request a Free Billing Audit Today →